Guidelines and norms for STDCs in NTEP
Guidelines and norms for STDCs in NTEPSTDCs are the Technical arm of the State TB Cell under the National TB Elimination Program. This document provides guidance around the various norms for establishing and for its ongoing activities and performance review.
Releases
| Release Date | Document Name | Status | |
|---|---|---|---|
| November 2003 | Document on State TB Training and Demonstration Centre (STDC) | Current | Click here |
| May 2023 | Guidelines and norms for STDCs in NTEP | Released | Click here |
| Current | Guidelines and norms for STDCs in NTEP | Live Document | Click here |
CIP Data
Guidelines and Norms for STDCs in NTEP, Central TB Division, MoHFW, Government of India 2023.
This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO license (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this license, you may copy, redistribute, and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that the Central TB Division, MoHFW, Government of India, endorses any specifc organization, products, or services. The use of the logos provided in this document is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons license. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the Central TB Division, MoHFW, Government of India. Central TB Division, MoHFW, Government of India is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the license shall be conducted in accordance with the mediation rules of the Government of India.
Suggested citation: Guidelines and Norms for STDCs. New Delhi, India; Central TB Division, MoHFW,
Government of India; February 2023. Available from: www.tbcindia.gov.in Cataloguing-in-Publication (CIP) data: Contributor author: Central TB Division, Ministry of Health & Family Welfare, Government of India; Coverage spatial: New Delhi, India; Date issued: Febrary 2023; Language iso: English; Publisher: Central TB Division, Ministry of Health & Family Welfare, Government of India; Rights: CC BY-NC-SA 3.0 IGO; Rights. uri: https://creativecommons.org/licenses/by-nc-sa/3.0/igo; Categories: Tuberculosis, STDCs, Health Systems; Title: Guidelines and Norms for STDCs in Delhi; Type: Electronic Publication; Rights holder: Central TB Division, Ministry of Health & Family Welfare, Government of India.
Sales, rights, and licensing: To submit requests and queries on rights and licensing, write to
ddgtb@rntcp.org.
General Disclaimer: All reasonable precautions have been taken by the Central TB Division, MoHFW,
Government of India to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The pupose of this document is to provide guidance on how STDCs should function/operate and is not legally binding. The responsibility for the interpretation and use of the material lies with the reader. In no event shall Central TB Division, MoHFW, Government of India be liable for damages arising from its use.
Live Document: Due to the evolving nature of the program the guidelines need to be updated frequently in accordance with it. This would mean that the content would be updated as and when any policy, procedure or technical instructions are changed.
Foreword and Acknowledgement
Foreword and AcknowledgementForeword

Capacity building of human resources is vital for achieving uniformity, effectiveness and high quality of services. State TB Training and Demonstration Centre (STDC) is the technical arm of the state TB programme. STDCs had undergone transformation over the years to technical units within the states to provide technical and managerial assistance to State TB Cell since the time of National TB Programme. To standardize the role of STDCs in NTEP,a reference guideline was prepared by the Central TB Division and the National Tuberculosis Institute (NTI),Bengaluru in 2003 for establishment and functioning of the STDCs in the states.
Strengthening of STDCs has been planned by NTEP under the ‘Build’ component of National Strategic Plan. With increased commitment for TB elimination by 2025, the NTEP has exhibited accelerated transformation since past few years. This has resulted into rapid changes across multiple domains/aspects of the NTEP. Thereis a felt need to strengthen roles of STDCs in various areas, especially training and supervision, monitoring andevaluation.
The updated guiding document of STDCs incorporates the current NTEP guidelines and also includes technological advances in the sphere of training and monitoring activities. I am sure that this guiding document will be of immense help to the STDC.
TB Harega, Desh Jeetega!
Dr. Rajejndra P. Joshi
Acknowledgement
The Guidelines and Norms for STDCs in NTEP (2023), the lead for which was taken by Central TB Division (CTD) and National Training Institute (NTI), Bengaluru to update the version published in 2003. This document is an end product of a series of consultations and meetings of the working committee held under the chairmanship of Director, NTI. The working committee is composed of technical experts from National Institutes, viz., National Tuberculosis Institute (NTI), National Institute of TB and Respiratory Diseases (NITRD), National Institute for Research in Tuberculosis (NIRT), development partners including The Union, World Health Organization (WHO), State Technical Experts including State TB Officers, STDC Directors, and Community representatives working in NTEP.
A Consultative Workshop was held at NTI Bengaluru in the presence of Central and State TB Officials in April 2022 to discuss on the felt need of updating the guiding document for functioning of State TB Training and Demonstration Centres (STDCs). An expert committee was formulated to deliberate on the recommendations and update the guiding document. Several meetings were organized physically and virtually in 2022 till 2023 by the CTD with technical and organizational support from National Institutes, The Union and WHO teams. The updated document henceforth, is built on the findings and recommendations of the STDC Baseline Assessment findings conducted by the USAID supported, The Union led iDEFEAT TB Project with the support of their consortium partner IQVIA.
Our deepest gratitude to Ms. Roli Singh, Additional Secretary & Mission Director, National Health Mission (NHM), MoHFW, GoI, Dr. P. Ashok Babu, JS (RCH & TB), Dr. Vineet Kumar Chadha (Advisor-NTEP) and Dr. K.S. Sachdeva, Regional Director (The Union) for the overall policy guidance and framework. The working on entire document was well supported and guided throughout by Dr. Rajendra P. Joshi-DDG (TB), GoI.
Our sincere thanks to Chair-Dr. N. Somashekar (Director-NTI) for his leadership and spearheading this initiative, Dr. Alok Mathur (ADDG-TB) for his constant support, Dr. Sanjay Kumar Mattoo (ADDG-TB), Dr. Raghuram Rao (ADG-TB), Dr. Nishant Kumar (Joint Director-Public Health) for their valuable inputs and Dr. Ravinder Kumar (TB Specialist-CTD) for his impeccable support throughout the entire process of updating the STDC guidelines.
We would also like to extend gratitude to Dr. Reuben Swamickan (Division Chief – Tuberculosis and Infectious Diseases – USAID India), Dr. Umesh Alavadi (Senior Health Advisor – Tuberculosis and Infectious Diseases, USAID India) for their expert guidance and whole hearted support to this initiative. We would also like to thank Dr. Ranjani Ramchandran (NPO-WHO), Dr. Malik Parmar (NPO-WHO), Dr. Kirankumar Rade (NPO-WHO) and Dr. Jyoti Jaju (Project Director-iDEFEAT TB Project, The Union) for overall support.
List of contributors
Dr. Somashekar N (Director, NTI Bengaluru), Dr. Alok Mathur (Addl. DDG-TB, CTD), Dr. Sanjay Mattoo (Addl. DDG-TB, CTD), Dr. Raghuram Rao (ADG-TB, CTD), Dr. Nishant Kumar (Joint Director-Public Health, CTD), Dr. Ravinder Kumar (Specialist-TB, CTD), Dr. Neeta Singla (NITRD), Dr. Tanmaya Talukdar (Professor & Head, LHMC, New Delhi), Dr. C. Ravi Chandra (Director-Training, NTI Bengaluru), Dr. Ranjani Ramchandran (NPO-WHO), Dr. Malik Parmar (NPO-WHO), Dr. Kirankumar Rade (NPO-WHO), Dr. S.K. Tripathi (NTI, Bengaluru), Dr. S. Uma Shankar (NTI, Bengaluru), Dr. Reena (Microbiologist, NTI), Dr. Niti Singh (Consultant Microbiologist, NITRD), Dr. Seenivasan Prabhu (Consultant Microbiologist, NIRT, Chennai), Dr. Sriram (Scientist D, NIRT, Chennai), Dr. Radhakrishnan (Consultant Microbiologist, NIRT, Chennai), Mr. Avijit H. Choudhury (WHO Country Office for India), Dr. Shibu Balakrishnan (NPO-WHO), Dr. Debadutta Parija (RTL-WHO), Dr. Kshitij Khaparde (RTL-WHO), Dr. D. Deka (RTL-WHO), Dr. Shivani Chandra (RTL-WHO), Dr. Sunil Kumar M (STO-Kerala), Dr. K.K. Chopra (Director-STDC, NDTBC), Dr. Md. Hanif (NDTBC), Dr. Anindya Mitra (Director-STDC, Jharkhand), Dr. A. Rajesham (Director STDC, Telangana), Dr. Varsha Rai (Director STDC, MP), Dr. P.R. Agarwal (Director STDC, Rajasthan), Dr. Sandeep Lavania (Director STDC, UP), Dr. Gopal Beri (Director STDC, HP), Dr. B.P. Panda (Director STDC, Odisha), Dr. N.D. Deshmukh (Director STDC, Pune), Dr. Pankaj Nimawat (Addl. Director, STDC Gujarat), Dr. Nirmala (Microbiologist-STDC KA), Dr. Neelam (STDC Bhopal), Dr. Saumya Dhawan (Microbiologist, IRL Bhopal), Dr. Tarun Patni (Microbiologist, IRL Ajmer), Dr. Bandana Choudhary (IRL Guwahati), Dr. S. Anand (National Consultant for TB Laboratories, WHO), Dr. Manu Mathew (The Union), Dr. Rakesh PS (The Union), Dr. R. Lakshmi (WHO-National Consultant), Dr. Shazia Anjum (WHO-SHQ, Karnataka), Dr. Sanjay Suryawanshi (WHO Consultant-Institutional Strengthening), Dr. Heena (NC-STDC Strengthening, The Union), Dr. Sivavallinathan Arunachalam (WHO consultant), Dr. Viral (National Consultant, The Union), Dr. Dheeraj Tumu (WHO Consultant), Ms. Sophia Khumukcham (WHO Consultant), Dr. Ranjeet Prasad (National Consultant, The Union), Ms. Richa Bharti (Technical Officer-ACSM, CTD), Mr. L.R. Sharma (State IEC Officer-HP), Dr. Paranjoy Bordoloi (State IEC Officer-Assam), Sashi Kanta Nayak (The Union), Ms. Himani Verma (Chattisgarh-TB Champion) and Adurrahman Urf Shahazad Ahmad, UP-TB Champion.
The CTD acknowledges the support of the technical experts involved at different stages of development of this guideline. We appreciate the contributions of all individuals who deliberated based on 2003 guidelines and findings of STDC baseline assessment (2022) and guided the way forward for updation of document, including present and former CTD colleagues and colleagues from various other departments. We are thankful to the committee members who participated in incorporating of recommendations put forward during follow-up meetings at NTI, Bengaluru and compilation of chapters including Dr. Ravichandra (NTI, Bengaluru), Dr. Uma Shankar (NTI, Bengaluru), Dr. K.K. Chopra (Director-STDC, Delhi), Dr. Gopal Beri (STO, Himachal Pradesh), Dr. Neeta Singla (NITRD, Delhi), Dr. Niti Singh (NITRD, Delhi), Dr. Mamata HG (NTI, Bengaluru), Dr. Rakesh P.S. (The Union), Dr. Manu E. Mathew (The Union), Dr. Sanjay Suryavanshi (National Consultant-CTD, WHO), Dr. Heena Goyal (National Consultant-CTD, The Union), Dr. Ranjeet Prasad (National Consultant-CTD, The Union).
Our deepest gratitude to Dr. N. Somashekar, Director-NTI, Bengaluru without whose support it would not have been possible to review the content and update the document. Towards the end, our heartfelt thanks to external members who could provide their valuable time to review the guidelines and share inputs for improvisation, including national professional officers from the WHO India, colleagues from non-government organizations and The Union Southeast Asia.
Introduction
IntroductionState Tuberculosis Training and Demonstration Centres (STDCs) are state-level strategic institutions in the National Tuberculosis Elimination Programme (NTEP) which is headed by an STDC-Director and acts as the knowledge hub in the state in relation to the TB programme. It supports the state in Programme Management by conducting its core activities of Supervision, Monitoring and Evaluation (SM&E) and Training in tuberculosis (TB) and NTEP. Apart from this, it also manages the Intermediate Reference Laboratory (IRL) and performs technical activities such as support in preparing the State Programme Implementation Plan (PIP), implementation and scale-up of new interventions, surveillance and TB burden estimation, ensure quality-assured laboratory services, conducting Operational Research (OR) and evolve the state strategic plan for TB Elimination.
The STDCs were originally established during the National TB Programme (NTP) and existed before 1998, as the Tuberculosis Demonstration and Training Centres (TDTCs). It was later re-designated as the State TB Training and Demonstration Centre (STDC) when Revised National Tuberculosis Control Programme (RNTCP) was launched. The STDC guideline was last released in 2003. It included Training, SM&E, Quality Assurance (QA) of TB Laboratory diagnostics and Advocacy, Communication, Social Mobilization (ACSM), and Operational Research as the major activities.
With the drive to accelerate progress towards TB Elimination, the NTEP has evolved and considerably expanded the range of TB services. The National Strategic Plan (NSP) of the NTEP envisaged the STDCs playing a significant role in building capacities of the NTEP cadres, General Health System and Private health care facilities/providers, along with SM&E of the programme and Operational Research. With the evolution of the TB programme, the functions of STDCs have also expanded. Thus, there was a felt need to revisit and revise the existing STDC guideline.
An STDC baseline assessment was conducted (2021–2022) with support obtained from United States Agency for International Development (USAID) supported iDEFEAT TB Project, to evaluate and document the current status and functioning of STDCs. It was observed that there was a wide variation in the capacity and functionality of STDCs in the country. Hence, there was a need to focus on revising the functional framework for STDCs.
With this context, this revision of the STDC guidelines seeks to formally update the previous guideline (2003) to match current programme operations and vision of “Ending TB”. By using the guideline, state NTEP administrators should try to align their STDC structure and functions and eventually bring uniformity in its minimum functions and performance across the country. It will also enable the NTEP leadership to evaluate the functioning of these strategic institutions and build capacity and strengthen them for optimal functioning.
Norms for establishing an STDC
Norms for establishing an STDCEvery State/Union Territory should have at least one functional STDC, established with infrastructure, equipment and human resource (HR, norms provided subsequently). It is preferably located alongside or nearby the State TB Cell (STC) at the State Headquarters/Capital, for administrative convenience, effective co-ordination and sharing of responsibilities.
In larger states, with a population of more than 5 Crore/more than 20 NTEP districts, they can establish additional STDCs or the single STDC at the state may be supported by additional Regional Training and Programme Monitoring Centre (RTPMC). The RTPMCs may be delegated with the responsibility of capacity building and SM&E activities. These additional centres would be governed by the single STDC at the state and may be resourced as per norms provided subsequently. RTPMCs function similar to STDCs, but they are placed away from the state headquarters based on the geographical and local considerations.
Integration with General Health System: Wherever there are no STDCs/RTPMCs as per the norms provided above, the state may decide to build the STDC/RTPMC in an appropriate existing state institution like the State Institute of Health and Family Welfare (SIHFWs) and regional training centres. Dedicated HRs, infrastructure and equipment as per NTEP norms may be provisioned to these institutions.
Human Resource
Human ResourceThe STDC works under the leadership of the STDC Director/Head of the Institution (STDC). She/he is an appropriately senior official from the state health system, preferably a TB specialist, or specialist qualified in Community Medicine or Public health or Microbiologist, having prior TB programme management experience, e.g., a former District TB Officer (DTO). In exceptional situation, the STDC Director/Head of the Institution may be from other specialties as per state policy. The STDC Director needs to be trained at National Level at a National Institute. This position is a regular and full-time post and the minimum tenure for a STDC Director is recommended for a period of 5 years, to ensure effective leadership at the STDC as well as to provide technical and operational support to the state in an efficient implementation of NTEP activities.
The staffing structure of the STDC should be given as mentioned in Figure 1. These positions may be regular positions from the State Health System or may be contractual staff as decided by the state health administrators. Three technical sections of the STDC – Training, SM&E, and the Intermediate Reference Laboratory (IRL) will each be trained at the National Institute. The Medical Officer-Training Division should be TB specialist, or specialist qualified in Community Medicine or Public health; Medical Officer-SM&E should be a specialist qualified in Community Medicine or Public health; while the IRL will be led by a Microbiologist.
The Medical Officer-Training is responsible for planning, organizing and conducting NTEP Training in co-ordination with other NTEP programme managers and medical college faculty. They ensure the availability of trained manpower and the conduct of need-based trainings at the district and sub-district level. They are supported by the Training Co-ordinator and a Statistical assistant. Together, they assess the training needs, prepare and execute the training calendar for STDC and district trainings across the state, according to the latest NTEP Training Guidelines in co-ordination with the DTOs and other staff.
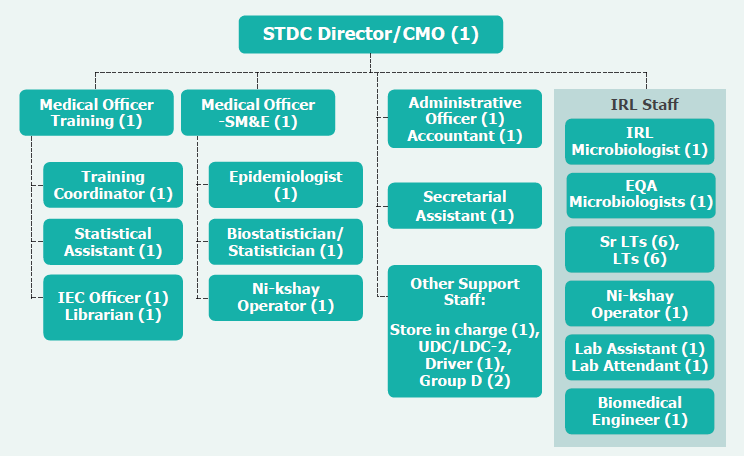
The Medical Officer-SM&E supported by an epidemiologist, biostatistician/statistician and Ni-kshay Operator, are responsible to conduct SM&E activities, at the state and district levels and ensure the optimum programme performance as elaborated in the NTEP-SM&E guidelines.
The IRL-Microbiologist is supported by the IRL staff as depicted in Figure 1 below. The IRL serves as reference Centre for diagnostic services and facilitates the establishment of decentralized facilities for TB diagnosis and infection detection. In addition, they will conduct laboratory-based hands-on training and External Quality Assessment (EQA) and Quality Improvement of decentralized laboratories functioning at the district and lower levels.
For administrative and financial functions, the STDC Director will be supported by an Administrative Officer, Accountant, Secretarial Assistant and other supporting staff (UDC-LDC). The Accountant manages the funds received for conducting the STDC activities and the Secretarial Assistant supports the STDC Director in general administration under the supervision of the Administrative Officer.
The RTPMCs need to follow the same staffing structure as the STDC, all of whom may report to the nodal STDC Director of the state. The senior most of the two medical officers at the RTPMC be in-charge of day-today administration.
When RTPMCs are built inside any existing state institutions, such as the SIHFW/Regional training institutions, the state may decide the organogram/reporting protocol for the staff of the RTPMC for administrative purposes. However, it is crucial to ensure that technical reporting to the STDC Director is maintained.
The above structure is the minimum HR expected for any STDC. The STDCs of larger states may need to be provided with additional staff, based on the load of activities. The norms for the qualifications and experience required for each of the STDC staff is mentioned in the latest HR norms and Terms of Reference (TORs), published by the Central TB Division (CTD).
Infrastructure and Equipment
Infrastructure and EquipmentThe STDC may preferably be located in the same premises where State TB Cell (STC) is situated or in close proximity for better co-ordination.
Every STDC/RTPMC needs to have adequate infrastructure and equipment to conduct its necessary functions. These include office rooms, training/meeting rooms, laboratory facility and residential/hostel facilities.
Office Rooms and Related Equipment
The STDC office rooms include the chamber of the STDC-Director, rooms for section in-charges (Training), SM&E and Microbiology divisions/units. It should also include appropriate space for the Training and SM&E section. It is desirable that the establishment section is located adjacent to the Director/Head of the Institution room/Chamber. STDCs/RTPMCs should also be equipped with adequate number of computers/laptops for each staff of the STDC.
Training/Meeting Rooms
- Auditorium with a seating capacity of approximately 50 people. It should be equipped with necessary audio-visual (AV) support.
- A separate room with a capacity of approximately 40–50 people for conducting district review and other administrative meetings.
- Three rooms with seating capacity of 15–20 people each. There needs to be separate class rooms wherever possible to have close interaction with each trainee during physical training.
Residential/Hostel Facilities
The number of residential facilities (approximately/at least 25 rooms) need to be provisioned based on the expected number of trainees undergoing concurrent training at the STDC. These may also be used for boarding and lodging of programme managers during review meetings. The hostel needs to have canteen, dining hall and housekeeping arrangements.
Modernized Training Unit
The STDCs/RTPMCs should be provided with the necessary equipment to effectively deliver trainings as per the requirements of the Modernized Training Strategy of NTEP. The Units may be installed in the auditorium/two training/meeting rooms as described above. Modernized Training Units at STDCs require facilities, such as:
- High-speed internet connectivity (either through a >50 MBPs leased-line or through a >200 MBPs Broadband/Fibre connection);
- Virtual meetings/knowledge dissemination setup (Virtual meeting service subscription, 3 Televisions, Camera, speakers, microphone);
- Interactive Digital Board (>65-inch diagonal size), or LCD Projector and screen (minimum 3 sets) along with Laptop or computer;
- Digital devices/tablets (minimum 40 sets) for the trainees;
- Portable AV equipment such as speakers, wireless microphones, laser pointers for trainings at satellite sites (minimum 2 sets).
Transportation
The STDCs need to have vehicle support to effectively deliver SM&E activities as per the policies of the State and for field-visit demonstrations to the trainees. If no vehicles are available, it may be hired from a suitable outsourcing agency.
The above training, residential and equipment facilities ideally be dedicated for the STDCs/RTPMC, but may also be shared with or borrowed from any regional/State Institute (SIHFW) or medical colleges as appropriate.
Infrastructure for IRLs
The IRLs established should have the following infrastructure:
- At least 2 rooms for sputum examination (Processing and Microscopy)
- Sample receipt room
- One room for sample opening with Biosafety Level-II facility
- TB containment laboratory
- Reagent and Media Preparation room
- Equipment area
- One washing and sterilization room
- Three physically separated rooms for conducting Line Probe Assay
- One room for Nucleic Acid Amplification Test activities
- One room for Laboratory Information Management System (LIMS), Ni-kshay Operator (DEO) and reporting
- Separate staff room with washroom for males and females
- One store room
- Walk in Cold room
The above infrastructure and related equipment and consumables need to follow Technical specifications provided by NTEP (Lab consumables, Equipment).
STDC Administration
STDC AdministrationThe STDC as an institution will function under the supervision of the STC. It will manage the RTPMCs and IRLs/ C&DST in the state. The STDC will have three sections: (1) the Training Section, (2) SM&E Section and (3) the IRL Section; each of which have a dedicated stream of activities in relation to conducting NTEP training, SM&E and laboratory-related work in the state. The personnel in these three sections will collaborate to provide all required technical assistance to the STC, such as PIP preparation and Operation Research.
The STDC will need to be empowered with adequate financial and administrative autonomy to conduct planned activities. The STDC will annually prepare an action plan prior to the State PIP process. The action plan has to include all training, SM&E, IRL and technical activities, such as operational research etc. The general norms for the quantum of each activity under each section should be based on needs/gap assessment keeping in mind the functions of STDC as detailed below. The action plan will also have to include the relevant budget with proper justification and timeline, and will have to be incorporated into the State PIP. Care has to be taken to ensure that the activities and budget include the necessary travel of STDC personnel within the state and other parts of the country for executing all its functions. The STDC staff may travel by hiring vehicles, through air/rail/ferry as appropriate, following the state National Health Mission (NHM) norms. However, the technical staff who are not entitled to travel by state norms, may be allowed to travel by air for attending National or Regional Level trainings/Workshops/Meetings/Evaluation visits, if it is an overnight journey or travel involving more than 500 km. They should be provided with timely permissions and TA/DA as per their entitlements/reimbursement of actual expenditure incurred with proper justification.
Once the PIP is approved, the total annual budget approved for the STDC and its divisions may be transferred to the STDC, to be used for approved activities under the annual plan.
Functions of STDC
Functions of STDCThe overall function of the STDC is to act as the technical arm of the STC. Acting as the technical arm, it directly is responsible for four major workstreams as motioned below:
- SM&E: STDCs would be performing continuous and real-time monitoring of programme performance through all the digital and physical information systems and reporting sources. Based on the same it would provide feedback and collect reports based on actions taken from the districts. To understand on ground scenario and compare programme vision and achievements it will also need to conduct supervisory visits and evaluate the current performance of the programme against the aspirations. The findings of the SM&E activities along with the necessary actions to be taken are to be communicated to the respective districts through the State Tuberculosis Officer (STO).
- Training: STDCs are expected to build the capacity of HRs in the programme, i.e., NTEP key personnel, general health system, medical college faculty and private health sector in relation to programme operations so that they are able to effectively deliver TB services and execute the roles expected from them.
- TB Laboratory (IRL): It will facilitate laboratory trainings and manage the resources at IRLs which in-turn is responsible for providing TB laboratory services, conducting hands-on laboratory-based training and for monitoring quality of laboratory services in the state.
- Technical Support: Technical support involves myriad activities, keeping in view TB epidemiology of state; prepare and evolve state-level TB elimination strategy and plan; generate evidence, prepare a need-based ACSM plan for all target groups and support them in the implementation of newer interventions.
STDCs need to optimally utilize virtual interaction platforms to deliver the above functions effectively (read guidance here).
The functions of STDCs are further elaborated under these four thematic areas.
Monitoring, Supervision and evaluation by STDCs
Monitoring, Supervision and evaluation by STDCsMonitoring, review, supportive supervision and evaluation are important to ensure that the programme is implemented as planned against the stated objectives and desired results. These are intensive technical activities and core function of the STDCs.
The STDCs need to lead activities in this area and support STCs. Designated nodal personnel (Medical officers, Epidemiologist, Statistician, Ni-kshay Operator) should be made accountable for regularly accessing data available from Ni-kshay and other programme information sources. They should also be involved in analyzing the data and preparing analyses and programme performance updates and reports for presentations (PPT) during review meetings. Based on the ongoing monitoring, review and supervisory activities, STDCs should regularly provide action-based feedback to districts and seek timely action taken report from them.
Details of the processes and approach to be followed in monitoring, supervision and evaluation are available in the NTEP Supervision and Monitoring Strategy (Click here).
The role of STDCs in SM&E are described below.
Programme Monitoring
Programme monitoring means collecting, compiling and analyzing data to determine progress of various activities under the defined thematic areas against the stated objectives at the district and sub-district level on real-time basis and periodically. Monitoring uses a set of core indicators and targets to provide timely and accurate information in order to review performance and inform progress and thus facilitating decision-making processes. This helps us to find timely solutions to the performance gaps- in each district. Programme monitoring is also of paramount importance for ongoing programme planning and implementation. Programme monitoring should be a routine function of STDCs.
The STDC need to access the Ni-kshay data and monitor the completeness, correctness and timeliness of data entry. They have to monitor the district wise performances on a day to day basis using the key indicators suggested by the NTEP. Further periodic Ni-kshay data analysis has to be undertaken for monitoring programme performance.
Whenever there is a significant under/over achievement or a remarkable variation of a particular outcome indicator, STDCs need to do a 'Root Cause Analysis' by looking at the input, process and output indicators related to it to find out the reason for the same. Using the Ni-kshay data, STDCs also should do the person, place and time analysis to gain insights to identify patterns and anomalies that may indicate reasons for poor or under achievement.
Based on the ongoing review, the STDC needs to
- Prepare and communicate the feedback with action points to the districts, as and when they find an issue in consultation with STO. The feedback shall include the detailed observations on key indicators, their Root Cause Analysis in short and suggested solutions to overcome the same.
- Obtain timely action taken reports and in-turn monitor the change in performance after the action.
- Purposively select Districts/ TB units (TUs)/ health facilities to be visited during supportive supervision, and evaluation.
- Identify priority performance themes and geographies (Districts/ TUs) to be reviewed during periodic review meetings.
Programme Reviews
Review meetings are conducted periodically aiming at identifying areas and actions for improving the programme performance. They are essential for quality improvement and sharing of best practices. STDCs need to support STC in the planning and conduct of monthly review meetings of the districts state in the following ways.
Planning and preparation for reviews is a crucial step that STDCs need to undertake in consultation with STCs. Thorough preparation and advance planning of agenda items (Programmatic themes and operational areas) needs to be done prior to the meeting based on inputs obtained from ongoing monitoring.
During the review meetings, STDCs should guide the discussions. such that they are based on objective criteria, and discussions progress in a consultative mode towards solutions. STDCs should ensure that the discussions are not limited only to outcomes, but also to inputs, processes and outputs. STDCs also should ensure that districts share their experiences, challenges, and best practices to facilitate cross-learning platform.
STDCs need to ensure that the review concludes with action-oriented feedback directed at specific responsible persons. All the feedback should be communicated to the responsible authorities within one week of the review meeting. All the emerging feedback from the review meeting should be consolidated as minutes meeting. STDCs also need to track the actions taken by all concerned based on the decisions made in the meeting/ feedback provided.
Supportive Supervision
Supervision is a systematic process for increasing efficiency of the health personnel by updating their knowledge, perfecting their skills, improving their attitudes towards their work and increasing their motivation. It is thus an extension of training.
Supervisory visits by STDCs should be a collaborative effort to identify problems and find solutions. The effort by the supervisory team, should be issue based and directed at provide ongoing support for solving problems and to overcome difficulties. Feedback provided during the visit should be constructive (with practical solutions) and not mere observations on performance. It should aim to build capacity of the health staff to implement the programme procedures correctly with high level of efficiency, to assess HR and training needs and to ensure data and service quality. At the end of the visit, the staff should be motivated and encouraged to effect solutions and bring improvements in programme performance.
Selection of districts: STDCs should conduct district wise supportive supervisory visits oriented towards the performance of the district as a whole, and in-turn evaluate performance and build the capacity/ competencies of the DTO and other NTEP staff and health functionaries. Selection of the district for supervision should be made based on the routine monitoring done by STDCs. Districts which require support need to be given preferences and shall be visited more frequently. However, selection should be done such that visits should cover all districts in the state at least once in a year.
Supervisory Team: A minimum of two members consisting of at least one medical officer from STDC/ RTPMC should visit the district for supportive supervision. And may be accompanied by STDC Director/ head of institution/ Senior Supervisory Staff from the state.
I. Conducting the visit in the district:
Key thrust programme operation areas for a supervisory visit should be purposively decided prior to the visit based on ongoing monitoring of the district performance. The institutions and corresponding staff to be visited may be decided based on the same. For example, if the reason for selection of a district is low treatment success rate from private sector, then high load private sector health facilities, current beneficiaries, their linked TU staff, and district PPM co-ordinator would be visited.
During the supervisory visit, data quality assessment in the selected focus areas should be done to assess correctness, completeness and timeliness. This would include verifying/ comparing data recorded in Ni-kshay (dates, categories, quantities) against the true/ actual value identified based on the context (recall/ records from beneficiary, hospital records etc.)
II. Visit Planning:
The Medical Officer (SM&E) of the STDC/ RTPMC should prepare in advance the monthly supervisory visit plan along with the focus areas for each district and include the same in Advanced Tour Program (ATP). A minimum of two districts should be visited by the STDC supervisory staff every month. For better efficiency, supportive supervisory visits could be clubbed with EQA visits by IRL. The monthly visit plan (ATP) should be submitted to the STDC Director before 25th day of the previous month. The STDC Director in-turn should communicate it to STO, the corresponding districts and the linked National Institute before the first official day of the month.
The supervisory visit should be made for at least for 3 days or more working days in each district. Based on the selected thrust area, institutions, staff and beneficiaries to be visited, the Medical Officer (SM&E) of the STDC may consult district to chalk out a suitable travel plan in advance. Based on the plan the Medical Officer (SM&E) needs to arrange suitable travel logistics with the approval of the STDC Director.
III. Output of a Supervisory visit:
At the end of the supervisory visit, feedback should be prepared and it should be specific action oriented along with supporting observations, with timelines. The observations and recommendations of supervisory visit should be discussed with the DTO and team and also for any administrative issues the districts/ State Health authorities may also be appraised. It should be submitted to the relevant authority(District TB officer, CMO, STO etc) who should take the action within 7 days of the end of the visit. STDCs should ensure that the each recommendation is an activity/task for the district/state to perform. STDCs should advocate to solve any issues requiring actions at the state level. STDCs should also monitor the actions taken against each feedback and close the feedback once the task is satisfactorily accomplished.
Internal Evaluation
Internal Evaluation forms an integral component of NTEP supervision and monitoring strategy. It acts as a tool to evaluate if good programme practices are adopted and quality services are provided to the community. These evaluations also offer an opportunity to look into all aspects of programme critically and swiftly. These activities help programme managers in understanding determinants of good as well as poor performance for replication of good practices in other districts and take appropriate measures for their improvement.
The STDCs should plan and lead the State Internal Evaluations. STDCs need to prepare a plan so as to cover all the districts in the state at least once in 3 years. Members of the team make plans and formats for evaluation should be based on the NTEP SM&E guidelines.
Training
TrainingOne of the core responsibilities of STDCs is to ensure that the health system is trained in delivering TB services and managing the programme effectively. In order to ensure adequate skill set for delivering high quality TB care on a continual basis, the staff may require to be trained in-depth at the time of induction into the system and provided with updates as and when necessary. A proportion of them may also need to be re-trained either periodically or based on their performance gaps/ competencies.
The STDC needs to directly execute training activities at the state level and also coordinate the execution of all the trainings of staff and trainers at the level of district and below. They may deliver training for the following purposes as mentioned below.
- Induction training: All the freshly recruited staff in the health system and deputed/ transferred into NTEP will require induction training in NTEP. Different categories of NTEP and General Health System staff have to be trained as per the relevant course curriculum (Modules/ hands-on training/ other guidelines) prescribed by NTEP for the respective cadre.
- Update training: This training should be provided as and when there is a change in programme guidelines or new operational processes are being introduced. For this purpose it is preferrable that all such newer initiatives may be compiled as fresh modules for the respective cadre and later integrated into the existing course at national level when they are revised.
- Refresher training: It is offered to the already trained officials either on their request or the official was trained long back and the supervisor or the official feels the need of training. Duration of this training will be similar to induction training or may be of shorter duration as per the need. Those who were already trained but were outside the programme for a significant period of time may also need to get a refresher training. (Periodically once in 3 years)
- Re-training: It is similar to Induction training for all the officials when a large sweeping change are adopted in the programme and the entire operational aspect is thoroughly changed or if an official needs to be retrained as per the assessment of the supervisor/ supervisory team.
The STDCs are required to train the trainers for all cadres in NTEP and facilitate and monitor cascade training for other staff at all levels of the health system in the state.
Planning Training
Planning TrainingEach year the STDC has to prepare the comprehensive annual training plan/calendar for the STDC and support the districts in preparation of their training plan and its inclusion in the PIP of the state. The training plan should be able to clearly state the number of batches of NTEP/ TB related training (with details of expected participants, facilitators, modalities used, start and end date, training locations/ venue, etc.) that will have to be executed in the state for all types of trainees including public, private, volunteers, medical college faculties, community and civil society members. This would include training at all levels including training of trainers and training at state/ district/ sub-district levels. Following are the activities to be done to prepare the annual training plan.
Maintain the HR and training database
The STDC has to maintain the database of all staff (including General Health System and Private sector) to be trained, cadre-wise pool of trainers and details of available training infrastructure at various levels in the state. The training database should contain details of:
- Sanctioned staff of different categories at various levels in the state and the current status (personnel posted in the respective position, regular/ contractual).
- Individuals posted at various positions including, personal profile, location of posting , their training log/history, competency feedback given by supervisors, and finally their training requirement based on position/ designations (such as pending training - induction/ re-training/ update, trained).
- Facilitators including log of Training of Trainers (TOTs) attended, details of the cadres that they are qualified to train, log of training feedback given by the participants.
- Infrastructure(venue/ location/ training halls) with equipment available.
The training database should be updated in real time. It is to be developed as an online tool and integrated with the Training MIS of the NHM (TMIS). Till such time a limited version of the database may be maintained as data in spreadsheets. (click here for sample format. Refer to annexure on instructions on filling this format).
Conduct a training need analysis: Using the regularly updated training database the STDCs should be able to undertake an assessment of the different types and quantity of training that they need to conduct in the coming year to ensure that the staff at different levels within the programme and of the Health System of the state are able to perform the duties/ roles expected of them. The assessment would also need to consider the priorities of training along with the time, resources and facilitators available to execute/ implement the training. Purpose/ aim of the needs assessment will be to estimate the NTEP related training load in terms of the number of personnel in various cadres to be trained in the different geographies of the state.
Build trainer resource pool: Based on the needs assessment and the gap in trainer requirements against the training load, the STDC needs to conduct relevant Training of Trainers (TOTs) for each cadre of staff. Trainers may be identified from a variety of sources including NTEP Staff, Medical Colleges, and National Institutes. TOTs can only be conducted by qualified Master Trainers for each cadre in the state.
Prepare the annual training plan: Using the database and based on the training need assessment, the STDC has to prepare its own annual training plan for induction/update/re-training and also support preparation of training plans including training calendar in the respective districts.
Prepare the Training Calendar: Based on the available capacity and priorities of the state, the STDC needs to prepare a training calendar. The Training calendar will list down the various trainings planned at all different levels based in a calendar/ Gantt chart format. The standard duration of each training needs to follow the NTEP's training guidelines for each type (induction/ retraining/update etc.). The facilitators for each batch of training, the dates and locations where in-person training/ demonstration/ evaluations would be conducted for each batch should be identified.
Update the Training Section of the PIP: Based on the training calendar prepared, the STDC should estimate the required resources (trainers, infrastructure, material, funds etc) on the basis of relevant NTEP norms(click here), keeping in view that the existing capacity at different levels. The STDC has to ensure that the funds required for the training are included in the PIP at the respective level. The STDC should also prepare relevant justifications for the conduct of the same and advocate for its approval. Based on the approved PIP, the STDC may try to fill the resource gaps through appropriate additional resources and ensure essential training is prioritized.
Training Execution
Training ExecutionThe STDC has to ensure that quality training is imparted to various cadres at different levels as per the Training calendar and the relevant CTD guidelines. the training material should include cadre-wise courses published by the CTD and should be shared with all the participants and other logistics. Some of the training material, especially for the peripheral field staff and community volunteers may be translated/back translated to local language and the STDC should develop the training material in local language.
Training of program managers [DTO, Medical Officer TB Control (MOTC), training of core NTEP staff [Senior Treatment Supervisor (STS), Senior Tuberculosis Laboratory Supervisor (STLS), District Programme Coordinator (DPC), Laboratory Technician (LTs) etc.], and training of all trainers in the state will be directly executed by the STDC. The STDC has to undertake the following steps with respect to the trainings directly conducted by it:-
- Reserve corresponding training venue/ infrastructure.
- Ensure enrollment of corresponding trainees in individual batches
- Inform and confirm the availability of facilitators
Training of staff like Microscopy-LTs , staff of general health system, private sector staff and health volunteers would be executed/ implemented at the district/ sub-district level under the overall supervision of the DTO. For the training conducted at the district/ sub-district level, the STDC should support in all aspects for conducting the trainings.
Some specialized training (e.g. training of Microbiologists and Sr.LT of IRL & CDST labs), and training of the state level program managers and Trainers would be conducted by the National Institutes. For this purpose the STDC should request linked National Institute to conduct TOT, training of state-level programme managers/ STDC staff as needed. STDCs may also facilitate nomination of trainers to be trained in upcoming TOT batches by the National Institute and facilitate their participation.
Sometimes additional trainings may needs to be organized over and above the annual training plan as per requirements of the state or as conveyed by CTD.
Monitoring and Evaluation of Training
Monitoring and Evaluation of TrainingAs training is being conducted through out the year the STDCs have to be able to generate and report the latest status of the training on demand. They should take action to ensure adequate performance against the plan. For this task the STDC needs to:
- Monitor the end-to-end execution process of each batch of planned training at STDC and other levels. This includes:
- monitoring of the batches initiated/completed as per the plan for various cadres/ geographies.
- monitoring the output of the training in terms of the proportion of trainees successfully completing the training.
- Take action for trainees who were unable to successfully complete training, by including them in the next available batch.
- Training feedback and quality assurance. This includes collating and analyzing the various quantitative/ qualitative feedback provided by the participants at the end of the course and translate the feedback into actions related to the trainer, training infrastructure and facilities, training content.
- At the end of each year before the next year's planning, evaluate the training conducted against the annual plan. Any shortfall may be accounted for during the subsequent year's training plan.
- Based on the evaluation STDCs should prepare the annual report of training conducted in the State and include it in the NTEP report of the state for future reference and review
Training Evaluation
It is imperative to evaluate the short-term effects and long-term gains of any training programme to update the knowledge and expected performance up gradation with respect to the changing programme strategies. This is especially important for the NTEP addressing TB having wide spread stigma prevalent in the community. This can be undertaken in association with linked National Institute periodically at least once in 2-3 years. (click here)
Management of the IRL
Management of the IRLAt the beginning of the RNTCP era, ZN microscopy was the only diagnostic technology available and STDCs were made in charge of monitoring and ensuring quality. Since then, laboratory services in the NTEP has been under continuous evolution and expansion. The programme has expanded to use a range of technology to detect both Mycobacterium Tuberculosis as well as resistance to the various anti-TB drugs. These include LED microscopy, polymerase chain reaction (PCR) based rapid molecular tests/ NAAT and C&DST. These tests have been increasingly scaled up and integrated into the TB Programme.
This evolution and expansion have resulted in laboratory services being a highly specialized Microbiological area. The IRL has evolved under the STDC as important institution in the NTEP. The IRL has the responsibility to ensure laboratory services for all technologies in the region are performing at the optimum standard and quality. In this context the STDC being the overarching institution for technical assistance to the state, it has to manage the IRL and ensure that it performs as per the expectations of the program. This includes:
- Completion of Microscopy/ NAAT Quality Assurance activities in the region as per plan. The Framework for implementing microscopy EQA available here.
- Facilitating the certification process and quality assurance of all linked C&DST Labs in the state.
- Co-ordinating the establishment of new C&DST labs in the state as per the needs, in consultation with CTD.
- Facilitating ongoing Lab Trainings at STDC
- Facilitating other ongoing programme functions in relation to laboratory services, mentioned in the corresponding sections.
Technical Assistance to State TB Program
Technical Assistance to State TB ProgramApart from the core routine activities of Training and SM&E, STDCs need to support the state by technically guiding the state TB programme.
1. Support and preparing the state strategy plan for TB Elimination: STDCs need to plan strategies and support the state to adopt state specific strategies and programme implementation approaches taking into consideration the TB epidemiology and health system strength.
2. Implementation of new interventions: Based on evolving programme guidelines issued by the CTD, STDCs need to support the state in implementation of new interventions in the state.
3. Support in preparing the PIP: The STDC based on the existing performance of the state and the needs identified based on the TB Elimination strategy of the state, needs to support the state and districts to prepare the PIP in such a way that the state and district NTEP is adequately resourced.
4. Advocacy: The STDC needs to advocate and obtain resources required for the state level strategy. Advocacy may be directed towards the sources such as the NHM, State Health System, Government representatives and Panchayati Raj Institutions, private and corporate entities, and even to the civil society and community at large.
5. TB Surveillance: The STDC should have a clear understanding of the status of the TB burden and epidemiology of the state through continuous ongoing surveillance activities. This may include activities such as conducting surveys, analysis of programme data and additionally collect data as per need. Based on this activity the state may apply for Sub-National Disease free certification.
6. Generate evidence for programme interventions in alignment with state strategy through suitable Operational Research, and by evaluating, documenting and disseminating the best practices by publishing related reports and periodicals.
7. Support Sub-national certification (SNC) for TB Elimination: STDCs need to support the SNC process.
Activities related to these processes need to be planned by the STDCs each year and budgeted in the PIP. Further details of each technical activity is provided below.
Preparation of state strategic plan for TB Elimination
Preparation of state strategic plan for TB EliminationIndia has a highly variant TB epidemiology and extreme difference in health system strength. One national strategy will not translate to effective on ground activities. STDCs need to technically support the state in identifying bold programmatic changes designed to accelerate progress toward "TB Elimination". STDCs based on its understanding of the State, need and context (TB epidemiology, strength of health system, resources available), needs to prepare and evolve action plan toward TB Elimination. The action plan while being in alignment with the interventions of the NTEP strategy, needs to consider the TB burden of the state, special population groups related to TB (vulnerable groups, migrants etc.). Based on this context the strategic interventions may add on to existing NTEP and may be directed towards
- Early and complete TB detection
- Correct and complete treatment
- Prevent new infection and break down to active TB
- Health system strengthening for TB care
Support Preparation of the State PIP
Support Preparation of the State PIPThe STDCs need to technically support STCs in preparing the annual action plan as per the state strategy for PIP preparation. This would include:
- Gap Analysis: The STDCs need to undertake district-wise gap assessment through analysis of the existing data, observations from the supervisory visits and periodic evaluations, a district-wise gap analysis need to be prepared. Gap analysis should highlight what are the major program gaps in terns of infrastructure, equipment, HR, activities and funds in each district.
- Identification of priority activities: Based on gap analysis, STDCs need to help the districts and state to identify the activities to be included on priority basis in the PIP of the respective district and state level.
- Capacity building and mentoring of district: STDCs should support DTO to prepare the PIPs of their respective districts including the micro-plan for each activity with number of beneficiaries and expected outcomes with proper justification. This may be done in a workshop mode before the preparation of the state PIP.
Medical Officer (SM&E) will be the nodal person who is responsible for the activity under the overall guidance of the Director STDC and STO.
Advocacy
AdvocacyThe STC has been provided ACSM Officer from the NTEP for carrying out and coordinating the ACSM activity in the State. The overall responsibility of ACSM activity would therefore lie with the STC. The STDCs would be required to provide technical inputs to make the ACSM activities more effective and also take certain advocacy activities themselves. The Key role of STDC is described as under: STDCs need to provide technical support to STC for:
- Advocacy with political and administrative officials at state and district level to obtain approvals on plans and secure necessary resources for the interventions in state TB elimination strategy. These may be from sources such NHM, State Health System, Government representatives, Panchayati Raj Institutions, private and corporate entities, and the civil society and community at large.
- Advocacy with scientific/ professional/ academic organizations/ institutions, Political leaders, Opinion leaders, non-governmental organizations (NGOs), TB Champions, AYUSH (Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homeopathy), Corporates and other government departments for implementation of the state TB Elimination strategy and for following Standards of TB Care in India
- Designing and Development of Advocacy and Information, Education and Communication (IEC) material in local language including contents for social media.
- Supporting the state and districts to develop annual ACSM plan.
- Dissemination of programme performance through publication of Bulletin / Newsletter every quarter.
- Design and implement “TB-Free Village” Certification as an advocacy initiative
TB Surveillance
TB SurveillanceIt is pertinent to have a clear understanding of the Epidemiology of TB in the state in terms of its burden (incidence and mortality rates) and its trends, identification of vulnerable populations, hot-spots of transmission of TB particularly of drug resistant TB, etc. The STDCs are expected to play a lead role in surveillance, by: -
- Ensuring correctness, completeness and timeliness of Ni-kshay data and other program data at all levels through day to day monitoring and necessary hand-holding.
- Periodic analysis of programme data.
- Collection and analysis of: a) Drug sales data and b) Schedule H1 data
- Mathematical modelling in collaboration with domain experts to forecast resource requirements, predict impact of specific interventions etc.
- Collect additional information, to understand/ estimate the time place and person changes in the burden of TB by undertaking surveys.
- Dissemination of the analytics at all levels within the state and outside the state.
The STDCs should co-ordinate and collaborate with Community Medicine Department of Medical Colleges, Public Health Institutes and Mathematics department of science Colleges including Indian Institute of Technology (IIT) and Indian Institute of Management (IIM). Epidemiologist will be the nodal person responsible for the activity.
Implementation of newer interventions
Implementation of newer interventionsSTDCs should support the state in strategically customizing and scaling up the new interventions and programme guidelines issued by CTD, from time to time, or as per state requirements for TB Elimination.
Specific roles of the STDC in this regard are as follows: -
- Mapping of all stakeholders for engagement
- Develop necessary training and communication material in local vernacular language.
- Develop and implement a training and capacity building plan.
- Prepare and implement the supervision and monitoring plan.
- Document the initial lessons and disseminate it for wider use.
- Support budgeting for implementation of the newer activities in the annual PIP.
Implementation and Operational Research
Implementation and Operational ResearchThe NSP encourages and promotes Operational Research to generate evidence on effectiveness of interventions and strategies aimed towards TB elimination. The STDC being the technical support arm of the STC should actively take a role in planning and conducting Implementation Research(IR)/ operational Research(OR).
The STDCs should independently plan and execute need-based Ooperational/ Implementation Research (OR). This would include:
- Identify research priority for the state to better achieve the program objectives in alignment with the Operational Research guidelines of NTEP.
- Disseminate research priority areas with the potential researchers, institutes, and agencies for the conduct of Operational Research.
- Organize capacity building sessions for interested program staff to design research studies and proposals in the form of an Operational Research workshops (Protocol Development, Report writing).
- Call for Proposals, review & approval of proposal in coordination with State Operational Research Committee
- Setup and host a formal Institutional Ethics Committee to review and approve any research proposals. They may also leverage any existing IEC at a co-located institution.
- Applying for and securing funds for executing research studies from external sources.
- Support state OR committee to execute approved studies
- Review progress of approved studies every quarter
- In coordination with Medical college task force, STDCs should also plan to conduct Operational Research dissemination workshop annually.
- Advocate for policy/ operational changes in the state and the country, based on Operational Research findings.
- Maintain a data base of all TB research (past/ ongoing/ published) from the state
- Evaluate and Document best practices in the state, and disseminate them by publishing related reports in periodicals/ journals for necessary programmatic uptake
The Epidemiologist of STDC will be the Nodal Officer for Operational Research related activities.
STDC should ensure that required budget for Operational Research related activities are proposed through the PIP mechanisms. It is essential for the STDC to have a concrete plan in terms of number of research projects proposed in the PIP.
Support Sub-National Certification
Support Sub-National CertificationUnder NTEP it is ongoing, regular & systematic surveillance conducted annually by CTD across the India. STDCs will support the conduct of annual SNC activities. In addition to that STDCs need to support SNC in the following ways
- Preparation and selection of districts for SNC claims including secondary data compilation and analysis
- Engaging with the available Public Health experts from Medical Colleges and other institutions.
- Supervision and monitoring the quality of the SNC process
- Training of volunteers.
Role of National Institutes in STDCs
Role of National Institutes in STDCsThe National institutes should play a significant role in supporting strengthening the STDCs in the states. They have to provide technical guidance and training for strengthening of STDCs in supporting State TB cell. The National Tuberculosis Institute (NTI), Bangalore, will be the nodal national institute for this purpose, while the other national institutes such as National Institute of Tuberculosis and Respiratory Disease (NITRD), New Delhi and National Institute for Research in Tuberculosis (NIRT), Chennai will support NTI, Bangalore for specific support functions across the country or regionally as suitable.
National institutes will advocate for and guide the establishment of STDCs as per the norms described earlier. Overall the National Institutes will support established STDCs in the following two ways:
A. Supervision Monitoring and Evaluation of STDCs:
The performance of STDCs must be monitored regularly based on its annual action plan by both State and Centre. From the central level NTI Bangalore, will support in monitoring the performance of STDCs on an on-going basis and provide quarterly report of the performance of the STDCs to CTD. This will include:
- Monitoring the performance of each STDC against their annual plan including the training status of the TB related workforce and the quality and status of feedback provided by STDCs to districts on their performance.
- National institutes will conduct need based supervisory visits to all the States and STDCs to cover all the states which are expected to have an STDC at least once in a year. They will provide action-oriented feedback for improvement.
- Provide feedback to the CTD, STDCs and STCs, regarding the performance and available capacity in STDCs, in an action-oriented manner.
-
Based on the Supportive supervision conducted across the country, NTI Bangalore needs to submit a compiled Quarterly report to CTD.
Refer to the checklist given at the end of the section on SME of STDCs, on the components to be included in SM&E of STDCs by the National Institute (Click Here).
- Advocate for prompt action from the state and Centre regarding the same.
B. Build Capacity and expertise:
Based on the monitoring and supportive supervision the NTI Bangalore will prepare a strategy to strengthening and build capacity of STDCs and plan activities annually. The strategy and activities should include, but not limited to the following areas:
- Induction Training of STDC and State level staff: All STDC and State level staff, including the STO and STDC director should be trained by the National Institutes. This should include training on Programme Operational areas and separate capacity building on their individual functions (such as Training, SM&E, Administration) based on the standard training materials provided by the Centre.
- Training of trainers (TOT): The National Institutes will host the resource pool of all Master trainers in the NTEP. Using the Master Trainers they are responsible for building the Trainer Resource Pool at the State level as per the needs of the state. The quantity of trainers required will be collaboratively identified by the state and the National Institute based on the load of training in the state. Whenever there is a shortfall in the resource pool, the state may request the NTI to conduct TOT, or such sessions may also be proactively conducted by the National Institute.
- Update training of trainers on changes or new programme implementation: Based on new program operation areas introduced or changes inducted by the CTD, the master trainer pool at the National institute should conduct Update training of all corresponding state level trainers.
- Theme-specific Training/ workshops.
- Surveillance and Data for action: This would include workshop for analysis and interpretation of data available from the Ni-kshay Information Ecosystem, and would be aimed to identify program performance gaps, conduct root cause analyses, and prepare action oriented feedback for improving program performance.
- State TB elimination strategy development workshops: These will be conducted by National Institutes on a periodic basis and will support the STDCs to develop State specific strategies, review and evolve them as per need.
- Operational research: National institutes will build the capacity of the STDCs in conducting Operational Research and by training and mentoring them.
Details of the conduct of training and content will be provided in the NTEP Training Guidelines.
Supervision, Monitoring and Evaluation of STDCs
Supervision, Monitoring and Evaluation of STDCsThe performance of STDCs must be monitored regularly on the basis of the annual action plan by both the state and centre.
The NTI, Bengaluru will support CTD in monitoring the performance of STDCs on an ongoing basis and provide a quarterly-biannually report of the performance of the STDCs to CTD. Along with any state NTEP review, CTD should also review the performances of STDCs.
Key Performance indicators for monitoring the functioning of STDCs are as follows:
- Proportion of training conducted by STDCs against planned.
- Proportion of supportive supervisory visits and EQA on-site evaluation (OSE) visits to district by STDCs against planned.
- Proportion of programmatic reviews with district facilitated by STDCs against planned.
- Proportion of state internal evaluation facilitated by STDCs against planned.
- Average number of action-oriented feedback, per district, provided by STDC in the quarter
- Proportion of actions taken report received against the feedback issued by STDCs (last 3 month status).
- Proportion of Operational research initiated by STDCs against annual plan.
- Proportion of Operational Research completed by STDCs against due date.
All supervisory and evaluation visits from centre to states such as Joint Supportive supervision, Central Internal Evaluation need to visit STDCs and review their performance.
Checklists for supportive supervision of STDCs/ RTPMCs are as follows:
- STDC/ RTPMCs established in the state/Union Territory as per norms and needs of the state.
- Staff for STDC/ RTPMC available as per norms
- Infrastructure and equipment including Modernized Training Units established at STDCs/RTPMCs as per norms
- Training plan of STDCs/ RTPMCs adequate to cover the health workforce in the state
- Training implemented in the state as per training guidelines
- Training conducted by STDCs are quality assured
- Training and training needs monitored by STDCs through TMIS
- SM&E plan of STDCs/RTPMCs compliant with guidelines
- SM&E activities conducted by STDCs as per the plan
- Technical assistance in the following domains provided by STDCs
- State-specific strategic plan prepared and revised timely
- TB Surveillance
- Preparation of PIP
- Advocacy
- Implementation of newer interventions
- SNC
- Operational Research
- Data in monthly reports submitted by STDC is correct and complete.
Annexures
AnnexuresBelow are annexures related to the Guidelines and Norms for STDCs.
Annexure 1:Framework for implementing EQA Laboratory network activities under NTEP
Annexure 1:Framework for implementing EQA Laboratory network activities under NTEPThere are three levels in EQA Laboratory network under NTEP
- National Reference Laboratories (NRLs), which are the Central Institutes designated under NTEP. They monitor EQA activities of STDCs/ State labs for the programme. There are six NRLs, viz., National Tuberculosis Institute (NTI) Bengaluru, National Institute for Research in Tuberculosis (NIRT) Chennai, National Institute for Tuberculosis and Respiratory Diseases (NITRD), Bhopal Memorial Hospital and Research Centre (BMHRC) Bhopal, Regional Medical Research Centre (RMRC) Bhubaneshwar and National JALMA Institute for Leprosy and other Mycobacterial Diseases, Agra. Each NRL will eventually monitor 8-12 STDCs/IRLs.
- STDC Laboratories will work as IRLs in the network. All States should have a State-level reference laboratory for EQA.
- The Microscopy Centres (MCs)/NAAT sites working for NTEP in the districts will be the Peripheral laboratories.
The three main activities under the NTEP EQA protocol are;
- On Site Evaluation (OSE): This evaluation is an important activity intended to evaluate whether the programme activities are being carried out i accordance with the recommended guidelines. Guidance is also provided for immediate corrective actions, wherever found necessary. OSE of the STDCs is done at least once a year by NRLs. DTCs (STLS) are evaluated once a year by STDCs and all MCs in the districts at least once a month by respective STLS. Importance will be given for taking action immediately at each level.
- Panel testing (PT): Panel testing is done mainly to check the staining and smear reading proficiency of LTs of STDCs and STLS of TUs. The Panel testing is not used as a routine for LTs working at TB Diagnostic Centres (TDC). Panel testing of LTs of STDCs and STLS will be conducted once a year under the supervision of the visiting NRL/ STDC team. A set of pre-fixed unstained manufactured slides are used per technician under supervision of the visiting NRL/ STDC supervisor.
- Blinded Rechecking of slides (RBRC): Blinded rechecking is the most important activity under the EQA programme. It determines the correctness of the smear results of LTs of MCs in an unbiased manner. It is not required for LTs of STDC as STDCs are expected to function at the supervisor level and are not required to perform patient related functions such as diagnosis and follow-up.
Methodology for all the three above mentioned activities is provided in detail in the revised NTEP EQA & DRS Protocols (refer to link)
The EQA for NAAT laboratories are undertaken annually by National Institute.
Annexure 2. Effective utilisation of virtual interaction facilities at STDC
Annexure 2. Effective utilisation of virtual interaction facilities at STDCAs an initiative to strengthen STDCs and enable them to perform their functions with better efficiency. The ECHO hubs have been established at STDCs. STDCs need to use these for improvement of programme efficiency and build the workforce capacity. Guidance for STDCs to design their virtual capacity building Programme and effectively utilise virtual knowledge hubs are as follows.
Virtual capacity building programs by STDCs
The knowledge hubs should be widely used by STDCs as a cross learning platform and for mentoring the health workforce at the periphery during the capacity building and programmatic reviews. Following are some of the ways it could be used.
- Training and Capacity Building: STDC is responsible for ensuring that the entire health system workforce is completely trained in NTEP. The STDCs could use knowledge hubs for training and capacity building in the following ways.
-
Regular training: STDCs lead the planning and implementation of regular and routine cadre-based training at all levels in the state for all healthcare staff working in the fight against TB in the state. This includes health system (Government or private), partners (NGOs, partner agencies etc) and other sectors. STDCs should effectively utilise Knowledge hubs for delivering the e- training courses for all cadres of including induction/ refresher/ update trainings. They need to prepare an annual training plan and decide which all courses could be scheduled as blended/ e- training through virtual platform. How such trainings could be conducted will be detailed in the training operations guidance under modernized training strategy under NTEP.
NOTE: Training in only virtual modes should be used only in situations where physical training cannot be conducted.
- Thematic Trainings: STDCs shall organize thematic trainings as and when there is a new programme or when there is an update of the guideline/policy or based on the local needs, or as directed by CTD such as PMTPT, PMDT, SNC, Partnership Guidelines, new features in Nikshay. STDCs shall identify the need and decide which all courses could be scheduled as e- training through the virtual platform.
- Dissemination of ongoing programme Updates: STDCs could plan regular or need based academic sessions at a fixed frequency for a specific target audience. This could be planned and designed based on local need. All such sessions need to be didactic with active involvement from the spoke institutions. For example, STDCs could plan a one-hour session for all TU level staff on every fourth Friday regarding TB and NTEP updates.
- Special advanced courses for building capacity of health workforce/managers/administrators: STDCs could design and implement special courses beyond the routine/ regular training based on felt need of the State, for improving the efficiencies of the health or non-health workforce as an ECHO program. For example, a course on soft skills or communication or leadership or management or operations research or financial management could be imparted to selected cadre of staff virtually.
- Continuing Medical Education: STDCs could plan CMEs on TB at fixed frequency for a specific target audience. STDCs could collaborate with State task force (STF) or professional associations for such programmes. For example, session for all post-graduates and interns of medical colleges in collaboration with STF or session for general practitioners in collaboration with professional associations on every second Tuesday. Topics for such sessions could be decided based on local needs.
- Case studies / Best Practices/ Cross learning Platforms: STDCs could also arrange a platform for facilitating experience sharing regarding success stories from field. Success stories could be any best practices or local solution to particular problems documented with some learning experiences. For examples DTOs can present about a case study about how they maintained case finding during COVID-19 pandemic period or how they engaged all sectors for TB or how they solved the issue of poor coverage of TB preventive therapy (TPT) among people living with human immunodeficiency virus (PLHIV). Such programmes could be conducted regularly on fixed days (eg. monthly every second Wednesday at 12:00pm).
-
- Programmatic Reviews and Supportive supervision: Programmatic reviews directed towards identifying problems and their solutions are an excellent opportunity for mentoring and improving capacity of district level and sub- district level staff. Data available through Nikshay and all other sources may be analyzed as prior preparation for the review and focused problem/ case-based approach may be used. These reviews need to be led and moderated by the STDC under the leadership of the STC.
- Periodic Reviews: These include monthly, quarterly, half yearly and annual review for the districts and other sub-levels organized by the STDC in consultation with STC These reviews could be directed internally within the NTEP or could be in collaboration with other programs such as National AIDS Control Organization (NACO) for cross learning and problem-solving activities.
- Need-based Thematic reviews: STDCs should conduct thematic reviews on periodically or based local needs. Such reviews will be focusing on one particular theme of the programme and will aim at building capacity of staff at field and solve problems at the field. These include reviews on PMTPT, PMDT, DBT, UDST, Private sector engagement, Pediatric TB Notification, Partnerships for TB Elimination, Finance, ACSM, Contact Tracing and so on.
- Virtual Supportive Supervision: STDC may use the virtual interaction platforms to conduct the supportive supervision activities aiming at handholding and mentoring of the staff at periphery in a virtual/ remote fashion. This includes virtual facility visit, physical examination of documents/ registers etc. Note that Periodic visits and regular supervision cannot be entirely replaced by virtual supportive supervisions.
- Additional need-based capacity building: In order to ensure that complex problems are solved timely, the ad-hoc meetings and reviews play an important role. It ensures timely actions for improving a specific indicator or improvement of programme of a particular district, institutions or staff.
Annual Planning of Virtual activities
Based on the above types of each of the above three types of activities the STDCs may plan an annual calendar of virtual events.
|
Sl No |
Date/ duration (Start end date sessions) with periodicity | Type of training/ Meeting | Topic | Spoke Institutions/ batch size and no. | Resource Persons |
Best Practices at STDCs
Best Practices at STDCs RichardSSTDC Pune Learning Corner- Introduction - Description of Best Practice
STDC Pune Learning Corner- Introduction - Description of Best Practice

Maharashtra State TB Training and Demonstration Centre (STDC) situated at Aundh, Pune is a glowing example of application of adult learning principles to impart effective training. The ‘learning corners’ used in STDC Pune, is an amalgamation of various modalities for training various cadres of NTEP staff.

A learning corner comprises a physical corner with audio-visual teaching aids (like display boards, information cards, creative presentations, audio recorded information etc.) on a particular topic, combined with detailed, self-reading material and facilitator-led exercises.
Rationale of the Practice & Implementation Strategy
Rationale of the Practice & Implementation StrategyRationale of the Practice: The learning corner is more of an approach, than a modality and is designed based on the adult learning principles of internal motivation, self-direction and is experience oriented and relevancy oriented. Training using multiple modalities and application of this knowledge for cadre-specific exercises and problem solving, are the highlights of this approach.
Implementation Strategy: Implemented from 2019 onwards, the learning corner was conceptualized by the then STDC Director Dr N D Deshmukh and supported by Training Coordinator Dr Asha Telang and team.
“The learning corner includes display of conceptualized material backed up with audiovisual aids in combination with other teaching modalities for effective learning. I would call these learning corners as teaching/speaking walls. My vision for a training programme is to benefit its participants in acquiring knowledge and bring about a positive change in their attitude and practice after the training. This is one of the successful experiments we have done in STDC Pune.”
DR NANDAKUMAR D DESHMUKH, FORMER DIRECTOR, STDC PUNE
Learning Corners
Learning CornersLearning Corners are present for all activities in the TB care cascade, including
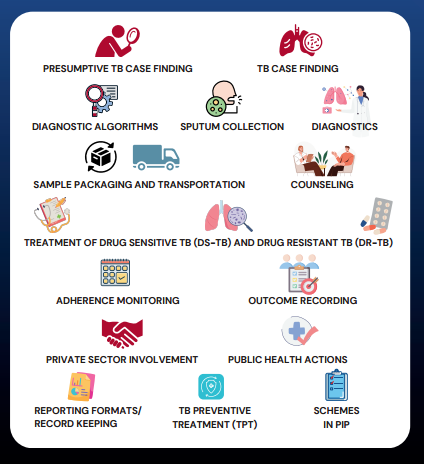
Customized training modules designed by the STDC team, as per the cadre getting trained, are disseminated prior to physical session. [1] [2] During the physical session, an orientation on key concepts is done by the facilitator using creative PowerPoint presentations. The participants then proceed to the learning corners established in the corridors of STDC building and undergo audio-visual experience of the relevant domains. For example, if the participants are learning about sputum collection and packaging, they would proceed to the relevant learning corner, read and understand the information board on the same, while the audio recording of the procedure of sputum collection and sample packaging will be played through speakers in the learning corner (Fig 2). The trainer/facilitator will also demonstrate the correct method of sample packaging using actual packaging materials. Fig 2 Learning corner at Pune STDC on sputum s ample collection & Fig 3 Learning corner at Pune STDC on sputum s ample collection.
The participants return to the classroom for in-depth discussions along with videos on the topic learnt and will be given exercise cards which will have a problem- solving exercise. For example, a case scenario will be described in the exercise card and the participant will be asked to do a cadre-specific problem solving (Fig 3), like filling the relevant reporting format for an STS trainee or describing the relevant treatment regimen for a medical officer trainee. The participants are then asked to apply the concepts learned to data from their own centre and present it among the trainees. This is applied and utility-based learning for each cadre, which empowers them to work confidently in the field.
“The learning corner was a new experience. The digital modalities employed in this training programme, especially the audiovisual content, helped me understand the key concepts in TB care cascade in a better manner. I also benefited a lot from the group discussions conducted, we learnt a lot of practical tips.” - Feedback of Trainee from STLS batch
Outcomes & Resources Utilized
Outcomes & Resources Utilized
Outcomes: Trainings for several batches of various cadres in NTEP, including District TB Officers (DTO), Medical Officers (MO), private doctors, Senior Treatment Supervisors (STS), Senior TB Laboratory Supervisor (STLS), pharmacists, PPM coordinators, TB Health Visitors (TBHV) and DOTS supervisors have been carried out successfully using this approach since 2019. Apart from appreciation from participants, the trainers/facilitators also feel that the approach has made their work more effective.

Resources Utilized: Learning corner was operationalized using pooled funds from the National Health Mission (NHM), the Maharashtra State Government, corporate social responsibility (CSR) funds of firms and a few personal donations. The training content was curated by the STDC team and printing of various IEC materials was supported by the State Health IEC department. The physical components of the learning corner including audiovisual system establishment cost about INR 2 lakhs and the training videos were produced as a CSR initiative.

“The learning corner approach helps us to break down the concepts into simpler terms and hence it becomes easier for the participants to internalize it. Also, the activity-based learning helps combat the monotony of classroom learning and participants are more receptive to our sessions.”- -DR ASHA TELANG, TRAINING COORDINATOR, STDC PUNE
STDC Tamil Nadu - Best Practice of Training the Health Volunteers to End TB in Tamil Nadu
STDC Tamil Nadu - Best Practice of Training the Health Volunteers to End TB in Tamil Nadu

Introduction
The National Tuberculosis Elimination Programme (NTEP) is dedicated to intensifying endeavors to end Tuberculosis in India. It provides comprehensive TB care services, fully aligned with the objectives outlined in the National Strategic Plan spanning from 2017 to 2025.1 Training Health Volunteers is essential in addressing misconceptions, effectively engage community, and increase community involvement in the fight against TB.2 The NTEP has created the ‘course for Health volunteers and Treatment supporters on NTEP’ through Modernize Training System (MTS).
Problem
Tamil Nadu Has identified Women Health Volunteers who are helping in the fight against Tuberculosis (TB).3 Their contributions include identifying TB cases, directing individuals suspected of having TB for testing, offering assistance in treatment to patients, and managing adherence to treatment plans. Additionally, they actively contribute to combating stigma and discrimination faced by TB patients within the community. They also play crucial role in all other health programs and activities including HIV and other health activities under primary health care.4
Reaching to a large number of health volunteers in short span of time for training is difficult and Also, Health volunteers need to be taught in their regional language and in a culturally appropriate manner. Evidence suggests that training program in Tamil for TB health volunteers is instrumental in fostering effective communication, community engagement, cultural sensitivity, and overall program success in Tamil Nadu.
1.RNTCP. National Strategic Plan for tuberculosis elimination. 2017
2.Government of Tamil Nadu. Tamil Nadu State Health Policy Vision 2030 “A promise towards Right to Health.” 2022
3.Knowledge base NTEP. Trainers Guide: Course for Health Volunteers on NTEP | Knowledge Base [Internet]. 2022 [cited 2024 Jan 16]. Available from: https://ntep.in/node/3557/revisions/12956/view
4. National TB Elimination Program. Tamil Nadu-National Tb Elimination Program Tamil Nadu-National TB Elimination Program Best Practices followed during the COVID 19 Pandemic. 2021.
Intervention & Methods followed for translating the standardized curriculum into Tamil
Intervention & Methods followed for translating the standardized curriculum into TamilIntervention:
Tamil Nadu state has decided to translate the NTEP approved ‘Course for Health volunteers and Treatment supporters on NTEP’ and train all the health volunteers using the modernized training system.
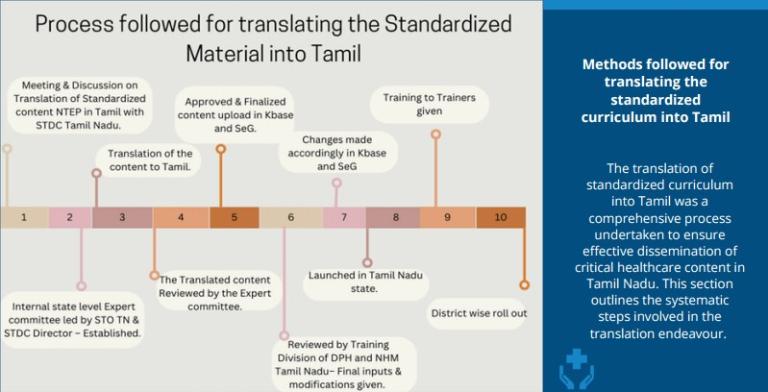
Figure 1: process followed for Translating the standardized Material into Tamil and Implementation strategy at the State and District level
Methods followed for translating the standardized curriculum into Tamil:
The translation of standardized curriculum into Tamil was a comprehensive process undertaken to ensure effective dissemination of critical healthcare content in Tamil Nadu. This section outlines the systematic steps involved in the translation endeavour.
| 1.Initial meeting and discussion | 2.Expert Committee Formation | 3.Translation of Content |
|
State TB Cell and STDC (State TB Training and Demonstration Centre) Tamil Nadu conducted the initial meeting and discussion involving key stakeholders to plan the translation process. Image

|
Established a state-level Expert Committee chaired by the State Tuberculosis Officer (STO) of Tamil Nadu and the Director of State TB Training and Demonstration Centre (STDC) to oversee the translation process, ensuring linguistic accuracy and cultural relevance. Committee included 8 other representatives who know programme very well and are fluent in Tamil Image

|
The Training curriculum was translated into Tamil by a team led State IEC officer. The translated contents were submitted on a timely basis to the expert committee for the review and feedback. The question bank for pre-test and post test questions attached to each chapter were also translated. Image

|
| 4.Expert Committee Review and Feedback Integration | 5.Configuration of training curriculum on Knowledge Base | 6.Review by the State Training division |
|
Expert committee members read the entire content together in physical mode and provided feedbacks on timely basis. The content creation team incorporated the suggestions and resubmitted it for approval. The expert committee had a total of 5 in-person meeting and one virtual meeting to finalize the content. Image

|
After approval, the final version of the translated content was configured into the Knowledge Base (Kbase). Home | Knowledge Base (ntep.in). NTEP Knowledge base is the subsystem of the modernized training system is the machinery to develop translatable multi-media training material. Image

|
The Training Division of the Department of Public Health (DPH) and the National Health Mission (NHM) in Tamil Nadu conducted a detailed review of the content focusing on cultural appropriateness and any potential conflicts with state norms. Image

|
7.Launch of the Course for Health Volunteers and Treatment supporters in Tamil Nadu :
The Modernized Training System for health volunteers was officially inaugurated in Tamil Nadu on March 13, 2023. The launch event, presided over by the Honourable Director of Public Health and Preventive Medicine DPH, marked a significant milestone in healthcare training initiatives.


8.Training of Trainers:
With the help of DTO, 2 Senior Women Health Volunteers and 1 DTTMO (District Training Medical Officer) from every district of Tamil Nadu were identified as Trainers. Entire pool of trainers were divided into two batches and 6 Hours ToT was conducted in two batches at state level on March 14th and 15th 2023.
9.District-Wise Roll-Out:
People to be trained were identified district wise, Training batches were created and scheduled through Learning Management System (WHO Swasth-E-Gurukkul) .In Phase -1, 5 districts have conducted trainings for Women Health Volunteers
Early Outcome: Training was conducted in several district, including Chennai, Coimbatore, Vellore, Villupuram, and Cuddalore. Across these locations, trainees consistently demonstrated improvement in their post-test scores compared to their pre-test scores. The total number of trainees attended were 454.
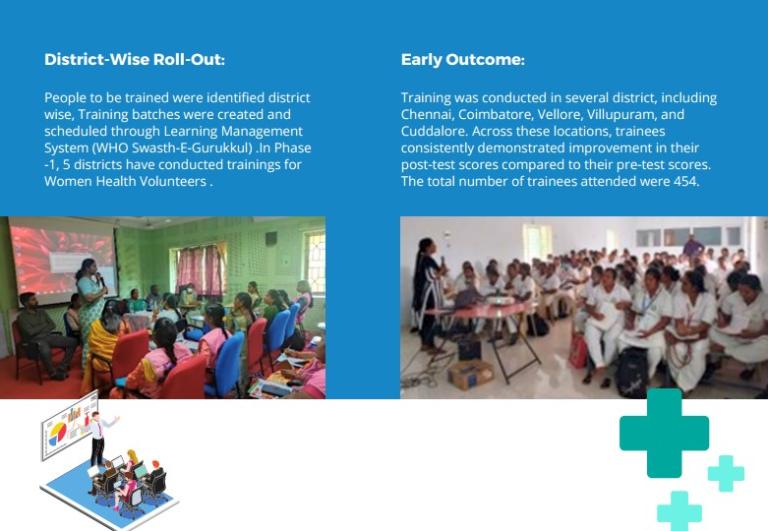
Details of training conducted for Women Health Volunteers
Details of training conducted for Women Health VolunteersTable 1 shows the number of Women Health Volunteers who successfully completed the course with the translated curriculum and the measures of change in pre-test and post test scores before administration of learning modules.
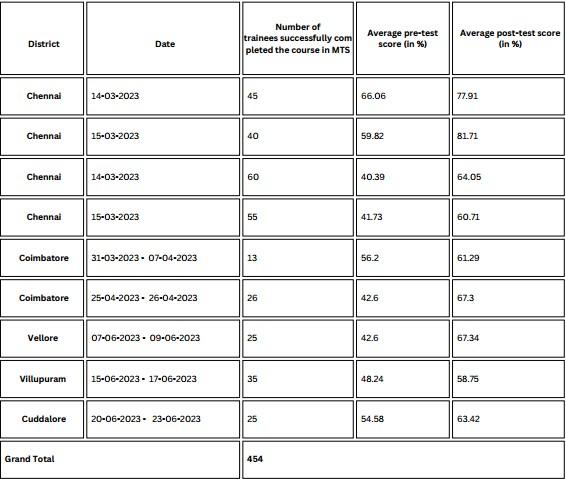

Conclusion
Conclusion
|
Image

|
STDC Tamil Nadu has demonstrated a system for translating the contents into regional language, which is replicable. Involvement of State Training Division, State Public Health Department and National Health Mission has ensured ownership from all the stakeholders. The meticulous execution of training using translated materials with adequate linguistic and cultural inclusivity, ensured that the health volunteers were able to obtain new learning and skills which are instrumental to their roles in TB prevention and care. Conducting the course in Tamil ensures that vital information is effectively communicated to the target audience. Experience from phase-1 has shown that it is feasible to train the health volunteer through modernize training system, This may help to reach out more number of health volunteers within short span of time. The "Tamil Nadu-Experience of Using the Modernized Training System for Training Health Volunteers" is a transformative initiative poised to make a lasting impact on TB prevention and care in the state. By combining cutting-edge technology with cultural sensitivity, this experience sets a benchmark for training of Health volunteers. |
STDC, Bhopal, Madhya Pradesh - Presence of State-of-the-Art Infrastructure in enabling to build a well-trained NTEP cadre: The story of STDC, Bhopal, Madhya Pradesh
STDC, Bhopal, Madhya Pradesh - Presence of State-of-the-Art Infrastructure in enabling to build a well-trained NTEP cadre: The story of STDC, Bhopal, Madhya Pradesh
Background:
Health systems can only function with health care workers; improving health service coverage and realizing the right to the enjoyment of the highest attainable standard of health is dependent on the availability, accessibility, acceptability and quality of health care workers.1 One of the key pre-requisites for providing quality healthcare services is building capacity of the health staff responsible for planning, implementing, monitoring and service delivery of the program.
Capacity building is defined as an approach to ‘the development of sustainable skills, structures, resources and commitment to improvement in health to prolong and multiply health gains many times over'.2 There are three identified distinctive dimensions to capacity building of health workforce3 :
Health Infrastructure or service development: Usually refers to the establishment of minimum requirements in structures, organizations, skills and resources in the program
Program maintenance and sustainability: Capacity to continue to deliver a particular program through a network of agencies.
Problem solving capability of organizations and communities: The capacity of health workforce to identify gaps/challenges in health programs and develop appropriate mechanisms to address them, either building on the experience with a particular program or as an activity in its own right.
The NTEP program released the revised guideline of the Roles and Functions of the STDCs in 2023.4 The guideline outlines the necessary infrastructure and facilities required to establish and function as an STDC across the country. Based on the guidelines, STDC Bhopal has been recognized to have set up high quality infrastructure and facilities for itself to enable enhanced quality training that is in tune with the guideline mandate. The document captures the infrastructure and facilities and its role in the capacity building of different cadres of workforce in the NTEP program.
“The STDC, Bhopal has established itself as an ideal training and capacity building institution. With its state-of-the-art infrastructure and

training equipment as well as other amenities required for a training centre, STDC Bhopal has been hosting national and regional level training workshops and gradually emerging as a training hub for cadres under the NTEP program”.
- Dr. Varsha Rai,
State TB Officer (STO)
STDC, Bhopal
Madhya Pradesh
1.World Health Organization (WHO): Health Workforce, website link: https://www.who.int/health-topics/health-workforce#tab=tab_1; Accessed on 27 August 2024
2. Hawe P, King L, Noort M, Jordens C, Lloyd B (2000) Indicators to Help with Capacity Building in Health Promotion. NSW Health Department, Sydney
3.Hawe P, King L, Noort M, Jordens C, Lloyd B (2000) Indicators to Help with Capacity Building in Health Promotion. NSW Health Department, Sydney
4.Central TB Division (Ministry of health Family Welfare, GoI): Related links : https://tbcindia-wp.azurewebsites.net/2024/08/07/guidelines-and-norms-f…; Accessed on 27 August 2024
History of the Establishment of STDC, Bhopal, Madhya Pradesh
History of the Establishment of STDC, Bhopal, Madhya PradeshThe state had witnessed the growth of the NTEP program from being a pilot project in two districts to an expanded program covering all districts by 2004. Important activities like undertaking testing and imitating patients on early treatment was being undertaken by the state with the objective of increasing case detection and improving treatment completion rates in the state. It was at this stage of the program progress in the state that under the leadership and close supervision of the Joint Director, TB and Director of National Programes and Principal Secretary, a proposal was initiated by the State TB Officer (STO) to have an independent infrastructure for the STDC, Bhopal. The process of establishing an independent building as the State Training and Demonstration Centre (STDC), Bhopal was initiated in 2006. The proposal was accepted by the state NHM office and an initial amount of Rupees 80 Lakh and subsequently an additional amount of 80 lakhs was allocated for construction of the STDC building and hostel accommodation. An additional amount of 2 crores was sanctioned in the year 2022 to complete the entire infrastructure of the STDC. Two medical officers from the State TB cell were given additional charge to ensure that the proposal was approved successfully within the given time through repeated and timely follow up including site visits Etc. The construction was done by the Public Works Department (PWD) in the state. The STDC, Bhopal is constructed on approximately 42 acres of land which also has the state TB hospital, the Intermediate Reference laboratory (IRL), a cancer hospital and the Food and Drugs office within this land. The land is owned by the state NHM.
Current Infrastructure of the STDC
Current Infrastructure of the STDCThe STDC is a three-story residential building and a functional basement with training/seminar room facilities, a separate computer room, residential rooms, kitchen and dining area etc. and a waiting room along with rooms for STDC staff including medical officers and a library. The ground floor has rooms for administrative persons, the kitchen and dining area, the first floor has training rooms (three Nos.), individual residential rooms and an open terrace with seating arrangement while the third floor houses the dormitories for male and female residents. All floors have washroom areas (separate toilets for males and females) and a drinking water cooler. The basement is largely used for storage purposes. The building has a lot of open area and a boundary wall. There is a small garden and kitchen garden within the premises. A detailed description of the infrastructure is provided below.
Rooms used for Training Purposes
The STDC has three kinds of rooms that are used for training purposes:
1.Seminar hall:
The biggest room is the seminar hall which is a 50 seated hall in a gallery style that also has a dais with a podium for all large sized trainings and other formal programs at the STDC. The gallery also has an interactive smartboard and three LED screens that are located strategically within the hall so that all participants have a proper view of the projection made on the smart board. The hall is also equipped with a good sound system including mics and an amplifier and a projector. The walls are panelled for sound proofing as well as for amplification and the floor is carpeted to reduce additional noise. There are four ACs in the seminar hall and an attached bathroom for males and females as well as a water cooler stationed right outside the hall.
2.Computer room:

The second hall is the computer lab which is smaller in size than the seminar room. This hall has designated desks and benches with computers (15 Nos.), screen and a smartboard with a stable internet system in place. The room has two ACs fitted. This room is primarily used for training cadres which require participants to use computers themselves during the training process (eg: medical officers and nurses).
3.Conference hall:

The smallest of the three training halls is the conference room. This room is designed to hold closed door meetings among small groups. It consists of a meeting table with a 20-seater seating arrangement around the table with an additional 20-seater arrangement. Other facilities in this room consists of a screen, LED and a hanging projector.
4.Residential Facilities:

The STDC, Bhopal, has hostel accommodation within the STDC building for those who attend training programs at the STDC. There are a total of 12 rooms at the STDC (8 rooms are on a double occupancy basis; 4 rooms are on a triple occupancy basis). A total of 28 persons can be accommodated in these rooms. In addition, there are two dormitory rooms (one for males and one for females). Each of these dorms have an arrangement of 10 beds with attached bathrooms, running hot water. All rooms for residential purposes have ACs, sufficient number of bathrooms with running hot water and provision for a common washing machine as well as laundry services on a self-payment basis. The rooms and dormitories are provided with appropriate number of study tables, chairs, wardrobe, a small pantry and a dressing table. All the rooms and the dormitories are well ventilated.
5.Dining Facilities:

The STDC has a large dining area and a fully functional kitchen that can cater between 50-60 persons at a point in time. The dining area has a seating arrangement for 40 persons at a time. There is a large sized fridge and a microwave in the kitchen/dining area for the purpose.
6.Rooms available for Administrative purposes by STDC staff:

There are dedicated rooms for the STDC director, medical officers and other staff of the STDCs. In addition, there are two rooms for administrative purposes of which one room has the Echo hub set up for meetings. There is a small library section in the second administrative room.
7.Other facilities/provisions available at the STDC:

The STDC has a solar panel with a capacity to generate 5 Kilowatts of energy equivalent electricity, regular water supply, steady internet (fibre plan of 40 GB) and routers in each floor for improved connectivity, and provision for a landline telephone connection. The expenditure incurred for electricity, internet and water is funded through the State Health society.
8.Human Resource available at STDC:

Currently, the STDC (including the IRL) has a total of 26 staff in place against a sanctioned human resource of 47 persons. The NTEP program provides 9 staff while 13 support staff (contractual) is provided by the NHM. The rest of the staff is positioned through the State health society.
9.Provision for Maintenance and Upkeep of the STDC:

While the STDC had received grants to set up the infrastructure across years, the regular maintenance and upkeep of the infrastructure is supported through income generated from hosting trainings for health cadres other than the NTEP staff. These include trainings conducted for ASHA, ANMs, nurses and Medical officers from block level facilities. The training halls and residential facilities are rented out to generate income that is used for regular maintenance of the building.
Key Learnings
Key Learnings
The primary learning from the establishment of the STDC, Bhopal, has been the high level of commitment shown by the senior authorities in prioritizing the establishment of the STDC, Bhopal. It is evident from the interviews conducted with multiple stakeholders at the state and review of relevant government documents that the importance of establishing a proper infrastructure for STDC was a ‘felt need’ by the senior officials to establish the NTEP program and improve on the quality of the service provisioning. This was in the context that the STDC staff were operating out of the two rooms from the TB hospital prior to the establishment of the STDC infrastructure. This impacted their ability to conduct regular trainings for the NTEP staff even as the program was expanding in the state and knowledge of the TB program was growing simultaneously.
Once the vision to establish the STDC was rolled out, it is important to note that the state ensured close supervision through the medical officers who were tasked to follow up on the construction and completion of the infrastructure. The entire process from conceptualizing to the construction of the building by different departments under the overall supervision of the highest official in the state for health worked to support each other to establish this institution building.


“The NTEP program in Madhya Pradesh has evolved immensely over the years and the establishment of an independent STDC building has added value to the optimal functioning of the program. As the program has evolved through the years, the NTEP cadre and their functions have also changed requiring them to be trained on the latest and updated knowledge. A designated residential training centre equipped with the latest technology and infrastructure has been key in ensuring a trained NTEP staff in the state contributing towards enhance program activities and outcomes. I hope other states in the country are encouraged from the story of the establishment of STDC, Bhopal and initiate their own STDCs”.
Dr. Varsha Rai,
State TB Officer, Madhya Pradesh
NTEP
STDC Agra,UP- From Planning to Practice: State TB Supervisor Training in Uttar Pradesh
STDC Agra,UP- From Planning to Practice: State TB Supervisor Training in Uttar PradeshSTDC Agra ensures uniform training covering over a thousand STS through meticulous planning
BACKGROUND:
The National Strategic Plan (NSP) 2017–2025 of the NTEP emphasizes that an "adequately staffed, trained, and motivated health workforce is essential to achieving the ambitious goal of ending TB.” In line with this vision, the NTEP envisaged the STDCs playing a significant role in building capacities of the NTEP cadres, General Health System and Private health care facilities/providers, along with SM&E of the programme and Operational Research. A key focus of the training strategy defined in the NSP for the programme is to not only to close gaps by addressing the need for a fully trained workforce but also to create a sustainable model that keeps staff updated on evolving policies and guidelines. This ensures the continuous flow of accurate information across all levels of NTEP personnel.
The Guidelines and Norms for STDCs in NTEP 2023, further underscore this responsibility, stating that ‘STDCs are expected to build the capacity of HRs in the programme, i.e., NTEP key personnel, general health system, medical college faculty and private health sector in relation to programme operations so that they are able to effectively deliver TB services and execute the roles expected from them.’ The guidelines recommend regular in-depth training at the time of staff induction, supplemented by updates as needed. Moreover, STDCs are tasked with preparing comprehensive training calendars annually and supporting district-level planning to align with the state’s Program Implementation Plan (PIP).
Recognizing this critical role, STDC Agra, meticulously planned and executed the uniform training of all 1017 Senior Treatment Supervisors (STS) in a two-year period, in line with the Guidelines and Norms for STDCs 2023. This document outlines the meticulous approach taken by STDC Agra to achieve this, highlighting the key steps in planning and delivering effective training that aligns with national priorities.
The Process
The ProcessThe task of training 1017 Senior Treatment Supervisors (STS) across the state demanded a well-coordinated and strategic approach from STDC Agra. To meet this challenge, the team developed a robust and comprehensive plan that laid the groundwork for successful implementation. This roadmap focused on gathering detailed trainee data, scheduling training batches, and ensuring timely communication and resource allocation. The planning phase set the stage for a seamless execution of the training program, ensuring every STS received the necessary knowledge, skills and support to contribute to the programme.
1. Planning
For ensuring uniform training of 1017 STS in the state, STDC Agra resorted to robust planning.
The first step was to create a comprehensive roadmap inclusive of following steps:
•Collection of Trainee information: The team meticulously crafted a detailed list of all STS personnel across the state, categorized by district. This was done based on the training planning tool prepared by Central TB Division (https://ntep.in/node/3614/BookPage/25-planning-tool) in collaboration with USAID supported The Union led iDEFEAT TB Project. This served as the denominator.
•Create Batches as per the resources available: Based on the infrastructure, dates and resource persons available, STDC Agra created batches for imparting the trainings.
•Assign Trainees to the various Batches: They assigned trainees to the various batches. Each training batch was scheduled perfectly to ensure the participation of every STS. Batches were created keeping in mind that the work on the ground is not to be affected. At the same time, STDC team ensured that no one was left behind.
•Communication/ Invitation to Trainees: Requisite and timely communication was sent out to the trainees allowing sufficient time to be prepared for taking the batches.
•Identification of the resources required for training: Medical Officers of the STDCs and WHO-consultants served as the resource persons for these training sessions. Resource persons were meticulously mapped against each batches to ensure their availability. Funds for the trainings were budgeted in Program Implementation Plan (PIP).1
•Localized Learning: Course for STS on NTEP approved by Central TB Division was a 40-hour curriculum including 11 modules and 43 chapters (https://ntep.in/node/3408). To enhance the understanding, STDC translated training materials into Hindi, making the content accessible for participants from diverse educational backgrounds.
2. Operationalizing:
STDC organized 32 training sessions for covering 1017 STS over two years, from August 2022 to April 2024. Out of these, 8 batches were undertaken using the modernized training system. The Modernized Training system entailed use of blended mode of classroom training such that the training was imparted using virtual technological mechanisms.
•Role of Training Co-ordinator: A dedicated training coordinator was appointed to oversee the entire process from start to finish. Their responsibilities included meticulously planning the training schedules in close collaboration with the State TB Cell and STDC, selecting and assigning facilitators, and ensuring the necessary resources—such as training venues—were in place. Additionally, the coordinator was tasked with organizing training batches, scheduling courses within the Learning Management Information System, monitoring the progress of the trainings, and keeping all key stakeholders regularly updated. This comprehensive role ensured smooth and efficient execution of the training program.
•Practical learning: The training was highly practical and immersive, featuring six-day induction sessions complemented by two-day refresher courses. Emphasis was placed on real-world applications, allowing participants to actively engage with the material. This hands-on approach not only deepened their understanding but also boosted their confidence in effectively applying newly acquired skills within their respective districts.
•Continuous Monitoring: The STDC assessed the effectiveness of the training by conducting pre- and post-tests through the Learning Management System (LMS), allowing for data-driven insights. Feedback was actively incorporated, enabling session adjustments to ensure continuous improvement and enhanced learning outcomes.
•Inclusivity at Its Core: The STDC created an accessible and supportive training environment by providing accommodations, meals, and logistical assistance for all participants, including individuals with disabilities. These efforts ensured an inclusive atmosphere, allowing everyone to fully engage in the learning experience
•Collaboration: The trainings were undertaken in collaboration with WHO NTEP Technical Support Network and The Union led iDEFEAT TB Project.
•Team Work: Under the chairpersonship of Director, STDC staff coordinated and implemented the training activities with a clear roles and responsibilities.
1. In the context of public health programs in India, especially under schemes like the National Health Mission (NHM), a PIP refers to a detailed annual plan that outlines the activities, interventions, budgetary allocations, and goals for implementing specific health programs at the state or district level.
Conclusion
ConclusionThe role of STDCs in building the capacity of NTEP personnel is pivotal to achieving the goals set forth by the National Strategic Plan 2017–2025. Through effective training and continuous updates, STDCs ensure that all cadres of NTEP staff are well-equipped to deliver high-quality TB care. STDC Agra’s meticulous planning and execution of training for 1017 Senior Treatment Supervisors over a two-year period serves as a prime example of how a structured, well-coordinated approach can successfully align with national priorities. STDC Agra has demonstrated the critical impact of robust training in enhancing TB service delivery and contributing to the broader goal of ending TB in India.
"Our success in delivering effective STS training in Uttar Pradesh was rooted in a systematic approach. First, we collected a detailed line list of all STS across the state. Then, we distributed responsibilities and ensured accountability for every task. Each team member had a specific role, whether it was planning the batches, addressing participant queries, or maintaining the training environment. We mobilized resources, created WhatsApp groups, and ensured seamless coordination—right from sending welcome emails to arranging guest lectures and hospitality. Every trainer was handpicked, and we had a dedicated person overseeing the entire training process. Finally, gathering feedback became essential for quality assurance and continuous improvement. This structure allowed us to deliver consistently high-quality training for all 75 districts for STS cadre”.
Dr.Sanjeev Lawania, Director, STDC Agra
STDC Delhi- Operational Research under NTEP: Learnings from New Delhi Tuberculosis Centre
STDC Delhi- Operational Research under NTEP: Learnings from New Delhi Tuberculosis CentreINTRODUCTION
India accounted for more than 25% of the global TB burden. To End TB, various interventions are planned by the Centre and State under the National Tuberculosis Elimination Program (NTEP).1 Operational Research is one of the requisites to generate continuous evidence to ensure state strategies are aligned well with the National Program. This evidence informs change in interventions or policy and optimize implementation of program activities to improve overall health outcomes.2
The National Strategic Plan for TB Elimination in India encourages and promotes Operational Research (OR) activity. Central Tuberculosis Division (CTD) has published areas and priorities for operational research at state, zonal and national level. The ‘Revised Norms and Guidelines for STDC’3 recommend STDCs to independently plan and execute need-based operational/implementation research and inform effectiveness of interventions at State.
However, most of the STDCs in the country are unable to conduct research activities due to underlying deficiencies in the systems or capacities. STDC Delhi has been conducting research studies regularly. Most of the projects have been conducted in collaboration with Indian Council of Medical Research (ICMR), National Institutes for TB, Medical colleges at New Delhi, Delhi TB-Association and development agencies like FIND (the global alliance for diagnostics), The UNION (International Union Against TB and Lung Disease), MRC-London (Medical Research Council), Centre for Equity etc. Around one-third of the total research projects undertaken by STDC Delhi in past 7 years are Operational research projects.
Since 2016-17, 102 research projects have been published as formal research papers, 56 of them have been published in the past 3 financial years. Some of the findings from these research studies have been incorporated into practice under NTEP. Findings from studies like National Sample survey for TB in 1950, eight longitudinal disease prevalence surveys conducted in domiciliary area of STDC Delhi for over 30 years, Active Case Finding (ACF) campaign in homeless pavement dwellers along Yamuna Pushta with mobile X-ray van supported by Medanta Medicity in Gurugram4 and prevalence of initial and acquired drug resistance and outcomes of Short-course chemotherapy (SCC) are some of them.
STDC Director and the staff has participated in 889 scientific events in last decade (since 2014-15) which has resulted in collaborations, cross-learning, funding and more research opportunities. The staff has gone an extra mile in presenting their research projects and findings at National (19) and International (13) scientific platforms. This document captures the experiences of STDC Delhi in conducting an operational research and key learnings. The enabling factors are listed in detail as an information for other STDCs to enhance replication and uptake.
STDC Delhi
Established in 1940 by Government of India and TB Association of India4 (TAI) jointly, officially known as New Delhi TB Centre (NDTBC) functioned as a model clinic for initiating organized domiciliary treatment for TB. In 1951, the center upgraded to first TB Training and demonstration center (TDTC) to provide training to health care workers and diagnostic referral center for five northern states until formal declaration as an STDC in 2005. Since then, STDC Delhi has been actively promoting operational research with the prime objective of evolving patient friendly and cost-effective treatment to people with TB. The details of the research activities and projects may be assessed from the annual reports published by STDC Delhi.4
1.https://tbcindia.mohfw.gov.in/wp-content/uploads/2023/06/5646719104TB_A…
2.theunion.org/sites/default/files/2024-06/Union OR to Improve Health Services 2nd 2024.pdf
3.https://tbcindia.mohfw.gov.in/wp-content/uploads/2024/08/Norms-and-Guid…
4.https://www.ndtbc.com/annual-report
Enabling Factors For Conducting Operational Research at STDC Delhi
Enabling Factors For Conducting Operational Research at STDC Delhi1.Human Resource: STDC Delhi developed its full-fledged sections in epidemiological, public health, statistical and administrative wing. The STDC director provides leadership and guidance to opportunities for conducting research. The Epidemiologist at STDC serves as the nodal officer for implementation of research. He is supported by a microbiologist and a biostatistician for monitoring collection and analysis of research data.
2.Capacity Building on OR: The key staff along with STDC Director completed their formal training in research methodology in 1990 and ‘How to do Operational Research?’ in 2005 at National Tuberculosis Institute, Bangalore.
3.Financial Resources: Along with funds earmarked for operational research in State NTEP funds, STDC Delhi shares experience of trying odds with every opportunity to fund its research. In last 10 years, more than 50% of the total researches were funded by State Operational Research Committee. In addition, some research projects are funded by ICMR or external agencies like MRC London, Corporates like Sandoz under corporate social responsibility (CSR). Funds earmarked for research studies are restricted to use under the same functional component.
4.Infrastructural capacity: Accredited with National Accreditation Board for Testing and Calibration Laboratories (NABL), the Intermediate reference laboratory (IRL) at STDC Delhi is equipped with Biosafety Level-3, Whole Genome Sequencing (WGS), second-line Line Probe Assay (LPA) and Liquid culture DST (drug-susceptibility testing) facilities. These make STDC Delhi a preferred site for research projects meant for multi-centric clinical trials, kit validation or validation of new diagnostic modalities4 in collaboration with RBIPMT (The Rajan Babu Institute of Pulmonary Medicine and TB), NITRD (the National Institute of TB and Respiratory diseases) or NIRT (National Institute for research in Tuberculosis, Chennai).
5.Orientation to potential researchers: STDC Delhi regularly conducts orientation workshops for potential researchers (DTO), faculty from various medical and nursing colleges, development agencies and corporate entities to sensitize on potential areas for operational research. Guidance on research tools to support good quality data collection is circulated.
6.Institutional mechanisms: STDC Delhi has established an institution level 7-member Scientific Advisory Committee, that reviews and finalizes the research proposals to be submitted to Operational research committee on behalf of STDC Delhi.
STDC Delhi has its own Institution Level Ethics Committee4 with members represented from TB Association of India, Delhi TB Association, State level Legal advisor, Community member, STDC itself and chaired by a Medical College faculty. The committee reviews the submitted protocols and provides ethical clearance based on the type of research involved.
7.Collaboration with State OR mechanism: STDC Delhi remains the focal point for organizing state task force meetings. The State Operational Research committee meets at STDC Delhi regularly to review and finalize the submitted proposals. Hence, any upcoming/ ongoing research is informed to STDC Delhi and priorities for conducting the same is facilitated. The State Task force also advocates for one thesis per medical college in a year to be undertaken by postgraduates.
8.Collaboration with TB Association of India (TAI): The staff of STDC Delhi provides managerial support to TB Association of India. They support the publication of the quarterly journal of TAI as members of editorial board4. Also, the faculty actively participates in annual conferences organized by TAI and supports in finalizing the scientific program and participating in the sessions. This provides an opportunity for STDC Delhi to create more awareness in their staff regarding current priorities of the national program, learnings from other states and dissemination of their research findings.
9.Maintaining a database of research studies: STDC Delhi documents the database (offline & online) of TB related (past and ongoing) research activity conducted in state. It is maintained as a part of the program annual report documented by STDC. It helps in wide dissemination of undergoing projects and provides an opportunity for collaboration, cross-learning or enhancement of research. Details of the research projects taken up in 2022-23 are listed in the annexure.
10.Dissemination of findings: STDC Delhi encourages use of various media to disseminate their research findings to the community at large. Around two-thirds of the total publication (71) is disseminated each through research publication or review article in past 6 years. This helps to keep the team motivated and continue to uptake further research projects.
Key Learnings
Key LearningsInvolvement of District Tuberculosis Officers: STDC Delhi encourages participation of District Tuberculosis officers (DTO) in conceptualization of research topics, implementation of research, training the project staff and monitoring the data collection. Inclusion of DTOs in the research team lays off any administrative issues related to data collection and absorption of research findings into practice.
Technical expertise from Medical College: STDC Delhi actively participates in approaching Medical College faculty for their technical expertise. Many research projects are planned in the form of thesis/ research work/dissertation as a part of the students’ medical programme curriculum. Having principal investigators or co-lead from the medical college adds value to the research topic and benefits the programme.
Supervision and Monitoring: Frequent supportive supervisory visits are conducted by STDC staff in the project area. The challenges in implementation are discussed and strategies are realigned, if necessary. The State OR committee regularly conducts mid-term review of the ongoing research studies.
Sustainable and resilient systems: STDC Delhi have worked around creating and sustaining institutional mechanisms that are not individual dependent. The processes for conducting an operational research at STDC Delhi has evolved and defined with time. It is elaborated in diagram below. Any operational research in the State is well informed to STDC and every activity is well coordinated with support from State TB Cell. The steps include collaboration with multiple stakeholders and their technical experts. Mechanisms to receive funds for research projects are well identified for smooth disbursement.
Process flow diagram for conducting Operational Research at STDC DELHI
Process flow diagram for conducting Operational Research at STDC DELHI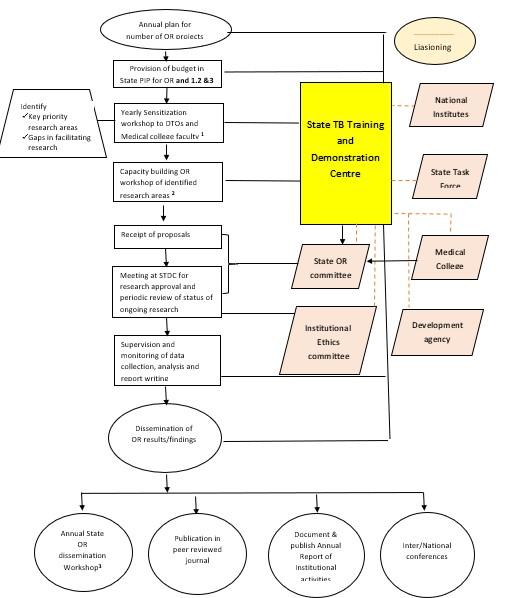
Few challenges on timely release of funds due to delay in in receipt of utilization certificate from other institutions have been reported. The STDCs need to anticipate such challenges and be prepared accordingly for smooth completion of research.
List of research activities supported by STDC Delhi in 2022-23
List of research activities supported by STDC Delhi in 2022-23|
S.no |
Title |
Study area |
Type of research |
Source of funding |
|
1 |
Mapping of Anti-Mycobacterial Drug Resistant Hotspots under NTEP in Delhi State |
STDC Delhi & TAI |
Operational Research |
Delhi State OR Committee |
|
2 |
TB prevalence & interventions for reducing TB and LTBI in high-risk key population of rickshaw driver & construction workers |
Selected districts of Delhi |
Operational Research |
ICMR |
|
3 |
Prevalence, risk factors and laboratory diagnosis of non-tuberculous mycobacterial (NTM) disease: A multicentric study |
IRL, STDC Delhi and 5 other sites in country |
Multi-centric trial |
ICMR |
|
4 |
Short intensified treatment for children with tuberculous meningitis (SURE) |
IRL, STDC Delhi and Kalawati Saran Children hospital, New Delhi |
Clinical Trial |
MRC, London, UK and National Institute of Health Research |
|
5 |
Evaluate the effectiveness, safety and tolerability of various Linezolid in combination with Bedaquiline and Pretomanid in Adults with Pre-Extensively Drug-Resistant or Treatment Intolerant/Non-responsive Multidrug-Resistant (MDRTI/NR ) Pulmonary TB in India. |
IRL, STDC Delhi and RBIPMT, New Delhi |
Clinical Trial |
ICMR |
|
6 |
Assessment of effectiveness of the 4-month Moxifloxacin containing daily regimen in the treatment of microbiologically confirmed new pulmonary TB patients |
IRL, STDC Delhi and TB Chest clinic at Lok Nayak Hospital |
Clinical Trial |
ICMR |