Proposed Components of CoE program
Proposed Components of CoE programProposed Components of CoE program are:
A. Establishment of Centre of Excellence (Hubs)
B. Identification of Spokes & establishing linkages
C. Clinical Support, Capacity building and mentoring of Spokes by the CoEs
A. Establishment of Centre of Excellence
A. Establishment of Centre of ExcellencePrerequisite for a CoE in DR-TB care is that it should have a well-functioning designated Nodal DR-TB center.
Potential institutions are expected to have the following essential features:
Sustained Patient load: The Centre due to its reputation and service offerings should attract a sustained patient load for DR-TB related services in both inpatient as well as outpatient departments.
Diagnostic services: Comprehensive diagnostic services for all types TB and DR-TB, including laboratory, radiology and clinical methods should be accessible to all patients reaching a CoE. Patients reaching the center should be receiving all necessary diagnostic services as per guidelines of NTEP.
TB Treatment Services: The Centre should have the capacity to initiate all types of drugs and regimen available under the program. All investigations for Pre-Treatment Evaluation should be available at a CoE. They should be able to assess progress to treatment and promptly adjust or modify the treatment regimen as per NTEP policy as needed. Facilities for managing DR-TB in patients of all ages, pregnancy and other special conditions should be present. In cases where patient shows indication of treatment failure/ intolerance or recurrence of TB/DR-TB and in complicated or difficult to treat cases, the center should have demonstrated ability to design appropriate regimen.
Adverse Drug Reaction management: The Centre should have demonstrated ability to manage all types of ADRs.
Comorbidity Management: There should be facilities to diagnose/ workup and manage all types of TB comorbidities.
Counselling Services: The Centre should have demonstrated ability to inform and educate patients about diagnosis, treatment, ADR and prognosis of their condition using services of expert counsellors in a non-discriminatory and inclusive manner.
Recording and reporting: The center should have a robust system for creating and maintaining clinical records of its patients along with prompt update of details in Ni-kshay as necessary.
Infrastructure and HR:
•Airborne infection control measures: These center should comply with AIC guidelines
•In-patient and Outpatient Services: The Center should have dedicated inpatient and outpatient departments for TB/ DR-TB. Outpatient services should be available throughout the week during working hours.
•Human Resources: The center should have in-place and trained human resources as per the guidelines and norms of NTEP with an emphasis on gender-responsive recruitment.
•DRTB Committee: It should also have a functioning DR-TB committee that meets regularly and provides consultation for its cases.
•Critical Care: The center should have ability to deal with critically ill patients due to TB/ DR-TB. This may be in the form of a TB Intensive Respiratory Care Unit with appropriate infection control measures and facilities or other methods to provide intensive life support and related care.
•Research and evidence generation: The Centre may be performing various studies or research in clinical, technological, operational or implementation areas.
It is highly desirable for a CoE to have the following
•Advanced diagnostic/ Treatment protocols –NTEP diagnostic and treatment protocols are standardized to consider the programmatic conditions that will be applicable all over the country. The Centre, however, may not be limited by this. They may adopt diagnostic and treatment protocols that are above and beyond the recommendations of the program to provide a more wholesome care to its patients. These need to be done with adequate approvals, documentation and rationale, and experiences from such extensions should be studied and published either as case studies/ series or as trials.
Advanced Surgical care in TB requires both advanced facilities and surgical expertise. These include lung resections, extra pleural thoracoplasty, extra pleural pneumolysis, thoracomyoplasty, pleurectomy and decortications of the lung; and so on.
Palliative care: The Centre should be able to provide appropriate palliative care for patients with disability, advanced disease or poor prognosis related to TB as described in PMDT guidelines 2021. The Centre should have demonstrated ability to perform palliative care either in-house or through linked services.
Pulmonary Rehabilitation: The Center should have a good pulmonary rehabilitation service catering to the needs of patients.
B. Identification of spokes & establishing linkages
B. Identification of spokes & establishing linkages10-15 spokes will be mapped with each CoEs. The selection of the spokes would be as per the following criteria: The spoke institution should be
•A designated Nodal/District DR-TB Centre
•Willing and committed to be a part of the spokes network of the concerned CoE.
•At a reachable distance with the CoE in a selected geography.
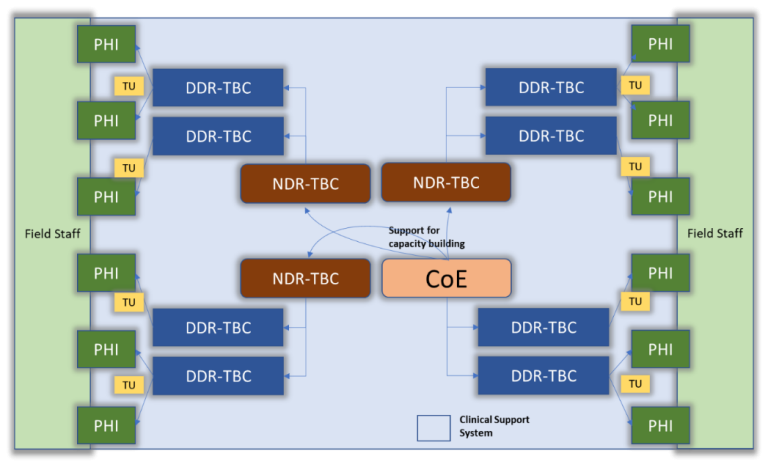
The CoEs (Hubs) will provide support to all the DR-TBCs (spokes) that are linked to it in a Hub and spoke model as illustrated below. The CoE and its linkages with NDR-TBCs will be identified by CTD in concurrence with the states and revised from time to time, as new CoEs are established.
C. Clinical Support, Capacity building & Mentoring of Spokes by Hub
C. Clinical Support, Capacity building & Mentoring of Spokes by HubThrough the hub and spoke model, the CoEs will provide support to the linked Spokes (N/DDR-TBCs) in
1. Clinical Support
2. Capacity building and
3. Mentoring.
The details are as follows:
1.Clinical advice: CoEs need to provide clinical advice for the Difficult to Treat cases referred to them form the NDR-TBCs. The referral will mostly be virtual where the provider seeks expert opinion from the CoEs through virtual interaction platforms. The virtual advice shall also be provided through the Difficult to Treat TB clinics (D3TC).
Suggestive models for Remote Clinical Consultations
i.Scheduled care model – Remote consultation that has a periodic predetermined schedule (Weekly/Monthly).
ii.Responsive (Reactive) care model or case based – Reactive, episodic care, which is usually unscheduled.
The above models can be delivered through two structures:
a)Clinical Consultation through Virtual Interaction Platforms: CoEs need to organize a monthly virtual session with spokes to discuss complicated cases. Such sessions could be organized more frequently based on the need.
b)Documented response to clinical queries: NDRTBCs can also raise queries to CoEs through their designated emails/other mechanisms. CoEs need to provide documented response to such queries.
.
Scope and advantages of Clinical Consultation through Virtual Interaction Platforms
•CoE will help in providing the expertise to remote areas and extend their expertise more quickly and easily by eliminating time and geographic barriers.
•CoEs and tertiary care facilities will be less over-burdened with premature/inappropriate referrals, if those cases could be managed properly at DDRTBCs. This will minimize patient inconveniences and promote quality care in a patient centric manner.
•Actionable decision support by CoEs would improve treatment outcome.
•Virtual Interaction Platforms will also establish a network between the mentoring and mentee in the region, thus going a long way in streamlining the process of referrals and back-referrals.
2.Capacity building: The CoE need to run regular capacity building sessions such as those related to newer updates, addressing common pitfalls/ gaps in DR-TB care practices, for its linked spokes. This need to be done as (a) monthly one-hour capacity building session through virtual interaction platforms (b) short courses and (c) observer ships programs
a)Capacity building through virtual interaction platform
Capacity building through virtual interaction platforms could be organized in the following ways.
1. Case based interactive sessions: Real-life case-based scenarios will be discussed by CoEs with spokes on a monthly basis to ensure cross-learning and selecting appropriate treatment plan.
2.Guidelines updates: Time to time update of recent management guidelines could be organized by CoEs
3.Strengthening Programmatic components: CoEs will use virtual interaction platforms to build capacity of spokes in programmatic components such as counselling, mental health assessment, managing co-morbidity, identification and management of ADRs, recording and reporting and data quality assurance.
4.Infection prevention and control (IPC): Sensitization of doctors and nurses towards AIC practices and biomedical waste management
b) Short Courses
CoEs to design and conduct short courses for the staff of spoke institutions. Courses need to focus mainly on the components which are not well demonstrated in DR-TB care such as TB Thoracic Surgery, Palliative care and Pulmonary Rehabilitation.
c) Observership
A plan for Observership can be developed by each CoE for the healthcare personnel of the spokes. Medical officers, nurses could be posted in the CoE for Observership.
Apart from the clinical exposure, these personnel will benefit from:
1. Participation in academic activities at CoE
2. Participation in daily bedside rounds by Faculty
3. Observation during bedside procedures and interventions
4. Separate daily academics for observers by Medical and nursing personnel can focus on:
a. Counselling for patients and family
b. Identification and management of Adverse Drug Reactions
c. Mental health and de-addiction
d. Nutritional status assessment & nutritional counselling
e. Air borne infection control
3.Mentoring to improve quality of care: CoEs need to mentor and handhold the spokes to improve in the quality of DR-TB service delivery.
This could happen through the following methods:
a.The CoEs need to conduct one-to-one virtual mentoring sessions with each of the identified spokes once in three months to address pertinent problems specific to that spoke and to suggest quality improvement interventions. During the mentoring sessions, staff of spokes could raise specific questions related to clinical or programmatic components of PMDT and seek guidance from the experts at CoEs. CoEs could also look at the areas for improvement in the spokes in relation to DR-TB care and suggest potential solutions. Key staff involved in patient care, NTEP Key staff of the institute along with administrative staff from spokes could participate in such mentoring sessions.
b.Experts from CoE need to attend the DR-TB review meetings organized by state/district NTEP, identify the potential issues, help them in performing a root cause analysis by looking at the processes and suggest possible solutions to address the priority problems.
c.Faculty from the CoEs need to visit the spoke institutions along with the state/ district NTEP officials during supportive supervisions and internal evaluations.