Best Practices at STDCs
Best Practices at STDCs RichardSSTDC Pune Learning Corner- Introduction - Description of Best Practice
STDC Pune Learning Corner- Introduction - Description of Best Practice

Maharashtra State TB Training and Demonstration Centre (STDC) situated at Aundh, Pune is a glowing example of application of adult learning principles to impart effective training. The ‘learning corners’ used in STDC Pune, is an amalgamation of various modalities for training various cadres of NTEP staff.

A learning corner comprises a physical corner with audio-visual teaching aids (like display boards, information cards, creative presentations, audio recorded information etc.) on a particular topic, combined with detailed, self-reading material and facilitator-led exercises.
Rationale of the Practice & Implementation Strategy
Rationale of the Practice & Implementation StrategyRationale of the Practice: The learning corner is more of an approach, than a modality and is designed based on the adult learning principles of internal motivation, self-direction and is experience oriented and relevancy oriented. Training using multiple modalities and application of this knowledge for cadre-specific exercises and problem solving, are the highlights of this approach.
Implementation Strategy: Implemented from 2019 onwards, the learning corner was conceptualized by the then STDC Director Dr N D Deshmukh and supported by Training Coordinator Dr Asha Telang and team.
“The learning corner includes display of conceptualized material backed up with audiovisual aids in combination with other teaching modalities for effective learning. I would call these learning corners as teaching/speaking walls. My vision for a training programme is to benefit its participants in acquiring knowledge and bring about a positive change in their attitude and practice after the training. This is one of the successful experiments we have done in STDC Pune.”
DR NANDAKUMAR D DESHMUKH, FORMER DIRECTOR, STDC PUNE
Learning Corners
Learning CornersLearning Corners are present for all activities in the TB care cascade, including
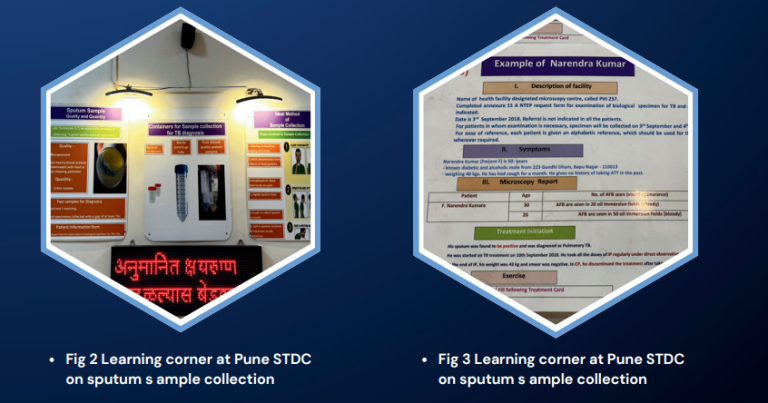
Customized training modules designed by the STDC team, as per the cadre getting trained, are disseminated prior to physical session. [1] [2] During the physical session, an orientation on key concepts is done by the facilitator using creative PowerPoint presentations. The participants then proceed to the learning corners established in the corridors of STDC building and undergo audio-visual experience of the relevant domains. For example, if the participants are learning about sputum collection and packaging, they would proceed to the relevant learning corner, read and understand the information board on the same, while the audio recording of the procedure of sputum collection and sample packaging will be played through speakers in the learning corner (Fig 2). The trainer/facilitator will also demonstrate the correct method of sample packaging using actual packaging materials. Fig 2 Learning corner at Pune STDC on sputum s ample collection & Fig 3 Learning corner at Pune STDC on sputum s ample collection.
The participants return to the classroom for in-depth discussions along with videos on the topic learnt and will be given exercise cards which will have a problem- solving exercise. For example, a case scenario will be described in the exercise card and the participant will be asked to do a cadre-specific problem solving (Fig 3), like filling the relevant reporting format for an STS trainee or describing the relevant treatment regimen for a medical officer trainee. The participants are then asked to apply the concepts learned to data from their own centre and present it among the trainees. This is applied and utility-based learning for each cadre, which empowers them to work confidently in the field.
“The learning corner was a new experience. The digital modalities employed in this training programme, especially the audiovisual content, helped me understand the key concepts in TB care cascade in a better manner. I also benefited a lot from the group discussions conducted, we learnt a lot of practical tips.” - Feedback of Trainee from STLS batch
Outcomes & Resources Utilized
Outcomes & Resources Utilized
Outcomes: Trainings for several batches of various cadres in NTEP, including District TB Officers (DTO), Medical Officers (MO), private doctors, Senior Treatment Supervisors (STS), Senior TB Laboratory Supervisor (STLS), pharmacists, PPM coordinators, TB Health Visitors (TBHV) and DOTS supervisors have been carried out successfully using this approach since 2019. Apart from appreciation from participants, the trainers/facilitators also feel that the approach has made their work more effective.

Resources Utilized: Learning corner was operationalized using pooled funds from the National Health Mission (NHM), the Maharashtra State Government, corporate social responsibility (CSR) funds of firms and a few personal donations. The training content was curated by the STDC team and printing of various IEC materials was supported by the State Health IEC department. The physical components of the learning corner including audiovisual system establishment cost about INR 2 lakhs and the training videos were produced as a CSR initiative.

“The learning corner approach helps us to break down the concepts into simpler terms and hence it becomes easier for the participants to internalize it. Also, the activity-based learning helps combat the monotony of classroom learning and participants are more receptive to our sessions.”- -DR ASHA TELANG, TRAINING COORDINATOR, STDC PUNE
STDC Tamil Nadu - Best Practice of Training the Health Volunteers to End TB in Tamil Nadu
STDC Tamil Nadu - Best Practice of Training the Health Volunteers to End TB in Tamil Nadu

Introduction
The National Tuberculosis Elimination Programme (NTEP) is dedicated to intensifying endeavors to end Tuberculosis in India. It provides comprehensive TB care services, fully aligned with the objectives outlined in the National Strategic Plan spanning from 2017 to 2025.1 Training Health Volunteers is essential in addressing misconceptions, effectively engage community, and increase community involvement in the fight against TB.2 The NTEP has created the ‘course for Health volunteers and Treatment supporters on NTEP’ through Modernize Training System (MTS).
Problem
Tamil Nadu Has identified Women Health Volunteers who are helping in the fight against Tuberculosis (TB).3 Their contributions include identifying TB cases, directing individuals suspected of having TB for testing, offering assistance in treatment to patients, and managing adherence to treatment plans. Additionally, they actively contribute to combating stigma and discrimination faced by TB patients within the community. They also play crucial role in all other health programs and activities including HIV and other health activities under primary health care.4
Reaching to a large number of health volunteers in short span of time for training is difficult and Also, Health volunteers need to be taught in their regional language and in a culturally appropriate manner. Evidence suggests that training program in Tamil for TB health volunteers is instrumental in fostering effective communication, community engagement, cultural sensitivity, and overall program success in Tamil Nadu.
1.RNTCP. National Strategic Plan for tuberculosis elimination. 2017
2.Government of Tamil Nadu. Tamil Nadu State Health Policy Vision 2030 “A promise towards Right to Health.” 2022
3.Knowledge base NTEP. Trainers Guide: Course for Health Volunteers on NTEP | Knowledge Base [Internet]. 2022 [cited 2024 Jan 16]. Available from: https://ntep.in/node/3557/revisions/12956/view
4. National TB Elimination Program. Tamil Nadu-National Tb Elimination Program Tamil Nadu-National TB Elimination Program Best Practices followed during the COVID 19 Pandemic. 2021.
Intervention & Methods followed for translating the standardized curriculum into Tamil
Intervention & Methods followed for translating the standardized curriculum into TamilIntervention:
Tamil Nadu state has decided to translate the NTEP approved ‘Course for Health volunteers and Treatment supporters on NTEP’ and train all the health volunteers using the modernized training system.
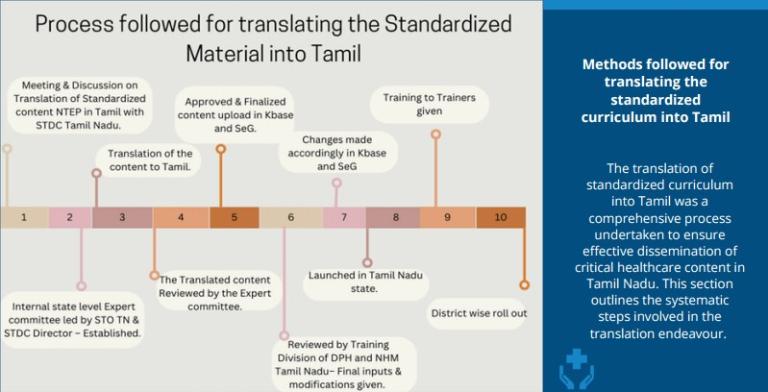
Figure 1: process followed for Translating the standardized Material into Tamil and Implementation strategy at the State and District level
Methods followed for translating the standardized curriculum into Tamil:
The translation of standardized curriculum into Tamil was a comprehensive process undertaken to ensure effective dissemination of critical healthcare content in Tamil Nadu. This section outlines the systematic steps involved in the translation endeavour.
| 1.Initial meeting and discussion | 2.Expert Committee Formation | 3.Translation of Content |
|
State TB Cell and STDC (State TB Training and Demonstration Centre) Tamil Nadu conducted the initial meeting and discussion involving key stakeholders to plan the translation process. Image

|
Established a state-level Expert Committee chaired by the State Tuberculosis Officer (STO) of Tamil Nadu and the Director of State TB Training and Demonstration Centre (STDC) to oversee the translation process, ensuring linguistic accuracy and cultural relevance. Committee included 8 other representatives who know programme very well and are fluent in Tamil Image

|
The Training curriculum was translated into Tamil by a team led State IEC officer. The translated contents were submitted on a timely basis to the expert committee for the review and feedback. The question bank for pre-test and post test questions attached to each chapter were also translated. Image

|
| 4.Expert Committee Review and Feedback Integration | 5.Configuration of training curriculum on Knowledge Base | 6.Review by the State Training division |
|
Expert committee members read the entire content together in physical mode and provided feedbacks on timely basis. The content creation team incorporated the suggestions and resubmitted it for approval. The expert committee had a total of 5 in-person meeting and one virtual meeting to finalize the content. Image

|
After approval, the final version of the translated content was configured into the Knowledge Base (Kbase). Home | Knowledge Base (ntep.in). NTEP Knowledge base is the subsystem of the modernized training system is the machinery to develop translatable multi-media training material. Image

|
The Training Division of the Department of Public Health (DPH) and the National Health Mission (NHM) in Tamil Nadu conducted a detailed review of the content focusing on cultural appropriateness and any potential conflicts with state norms. Image

|
7.Launch of the Course for Health Volunteers and Treatment supporters in Tamil Nadu :
The Modernized Training System for health volunteers was officially inaugurated in Tamil Nadu on March 13, 2023. The launch event, presided over by the Honourable Director of Public Health and Preventive Medicine DPH, marked a significant milestone in healthcare training initiatives.


8.Training of Trainers:
With the help of DTO, 2 Senior Women Health Volunteers and 1 DTTMO (District Training Medical Officer) from every district of Tamil Nadu were identified as Trainers. Entire pool of trainers were divided into two batches and 6 Hours ToT was conducted in two batches at state level on March 14th and 15th 2023.
9.District-Wise Roll-Out:
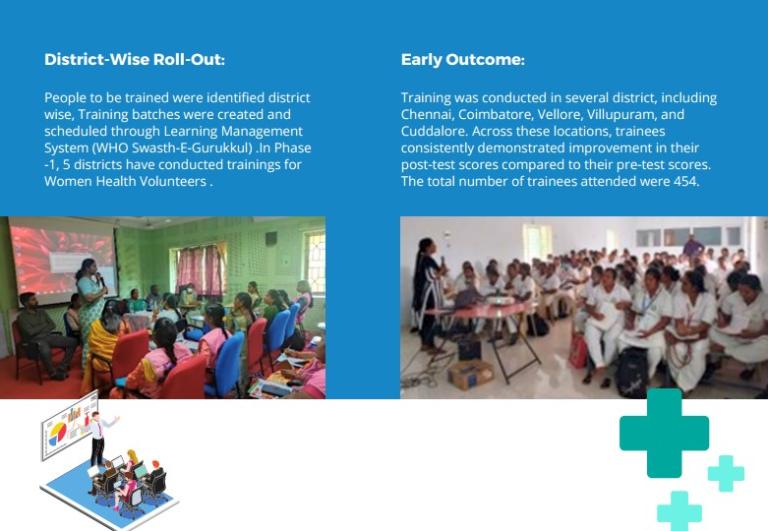
People to be trained were identified district wise, Training batches were created and scheduled through Learning Management System (WHO Swasth-E-Gurukkul) .In Phase -1, 5 districts have conducted trainings for Women Health Volunteers
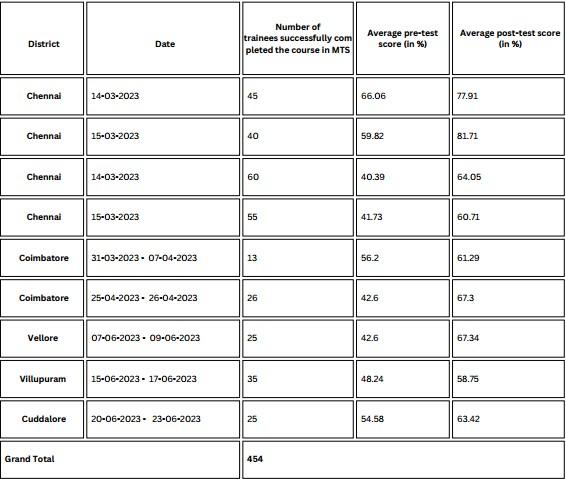
Early Outcome: Training was conducted in several district, including Chennai, Coimbatore, Vellore, Villupuram, and Cuddalore. Across these locations, trainees consistently demonstrated improvement in their post-test scores compared to their pre-test scores. The total number of trainees attended were 454.
Details of training conducted for Women Health Volunteers
Details of training conducted for Women Health VolunteersTable 1 shows the number of Women Health Volunteers who successfully completed the course with the translated curriculum and the measures of change in pre-test and post test scores before administration of learning modules.

Conclusion
Conclusion
|
Image

|
STDC Tamil Nadu has demonstrated a system for translating the contents into regional language, which is replicable. Involvement of State Training Division, State Public Health Department and National Health Mission has ensured ownership from all the stakeholders. The meticulous execution of training using translated materials with adequate linguistic and cultural inclusivity, ensured that the health volunteers were able to obtain new learning and skills which are instrumental to their roles in TB prevention and care. Conducting the course in Tamil ensures that vital information is effectively communicated to the target audience. Experience from phase-1 has shown that it is feasible to train the health volunteer through modernize training system, This may help to reach out more number of health volunteers within short span of time. The "Tamil Nadu-Experience of Using the Modernized Training System for Training Health Volunteers" is a transformative initiative poised to make a lasting impact on TB prevention and care in the state. By combining cutting-edge technology with cultural sensitivity, this experience sets a benchmark for training of Health volunteers. |
STDC, Bhopal, Madhya Pradesh - Presence of State-of-the-Art Infrastructure in enabling to build a well-trained NTEP cadre: The story of STDC, Bhopal, Madhya Pradesh
STDC, Bhopal, Madhya Pradesh - Presence of State-of-the-Art Infrastructure in enabling to build a well-trained NTEP cadre: The story of STDC, Bhopal, Madhya Pradesh
Background:
Health systems can only function with health care workers; improving health service coverage and realizing the right to the enjoyment of the highest attainable standard of health is dependent on the availability, accessibility, acceptability and quality of health care workers.1 One of the key pre-requisites for providing quality healthcare services is building capacity of the health staff responsible for planning, implementing, monitoring and service delivery of the program.
Capacity building is defined as an approach to ‘the development of sustainable skills, structures, resources and commitment to improvement in health to prolong and multiply health gains many times over'.2 There are three identified distinctive dimensions to capacity building of health workforce3 :
Health Infrastructure or service development: Usually refers to the establishment of minimum requirements in structures, organizations, skills and resources in the program
Program maintenance and sustainability: Capacity to continue to deliver a particular program through a network of agencies.
Problem solving capability of organizations and communities: The capacity of health workforce to identify gaps/challenges in health programs and develop appropriate mechanisms to address them, either building on the experience with a particular program or as an activity in its own right.
The NTEP program released the revised guideline of the Roles and Functions of the STDCs in 2023.4 The guideline outlines the necessary infrastructure and facilities required to establish and function as an STDC across the country. Based on the guidelines, STDC Bhopal has been recognized to have set up high quality infrastructure and facilities for itself to enable enhanced quality training that is in tune with the guideline mandate. The document captures the infrastructure and facilities and its role in the capacity building of different cadres of workforce in the NTEP program.
“The STDC, Bhopal has established itself as an ideal training and capacity building institution. With its state-of-the-art infrastructure and

training equipment as well as other amenities required for a training centre, STDC Bhopal has been hosting national and regional level training workshops and gradually emerging as a training hub for cadres under the NTEP program”.
- Dr. Varsha Rai,
State TB Officer (STO)
STDC, Bhopal
Madhya Pradesh
1.World Health Organization (WHO): Health Workforce, website link: https://www.who.int/health-topics/health-workforce#tab=tab_1; Accessed on 27 August 2024
2. Hawe P, King L, Noort M, Jordens C, Lloyd B (2000) Indicators to Help with Capacity Building in Health Promotion. NSW Health Department, Sydney
3.Hawe P, King L, Noort M, Jordens C, Lloyd B (2000) Indicators to Help with Capacity Building in Health Promotion. NSW Health Department, Sydney
4.Central TB Division (Ministry of health Family Welfare, GoI): Related links : https://tbcindia-wp.azurewebsites.net/2024/08/07/guidelines-and-norms-f…; Accessed on 27 August 2024
History of the Establishment of STDC, Bhopal, Madhya Pradesh
History of the Establishment of STDC, Bhopal, Madhya PradeshThe state had witnessed the growth of the NTEP program from being a pilot project in two districts to an expanded program covering all districts by 2004. Important activities like undertaking testing and imitating patients on early treatment was being undertaken by the state with the objective of increasing case detection and improving treatment completion rates in the state. It was at this stage of the program progress in the state that under the leadership and close supervision of the Joint Director, TB and Director of National Programes and Principal Secretary, a proposal was initiated by the State TB Officer (STO) to have an independent infrastructure for the STDC, Bhopal. The process of establishing an independent building as the State Training and Demonstration Centre (STDC), Bhopal was initiated in 2006. The proposal was accepted by the state NHM office and an initial amount of Rupees 80 Lakh and subsequently an additional amount of 80 lakhs was allocated for construction of the STDC building and hostel accommodation. An additional amount of 2 crores was sanctioned in the year 2022 to complete the entire infrastructure of the STDC. Two medical officers from the State TB cell were given additional charge to ensure that the proposal was approved successfully within the given time through repeated and timely follow up including site visits Etc. The construction was done by the Public Works Department (PWD) in the state. The STDC, Bhopal is constructed on approximately 42 acres of land which also has the state TB hospital, the Intermediate Reference laboratory (IRL), a cancer hospital and the Food and Drugs office within this land. The land is owned by the state NHM.
Current Infrastructure of the STDC
Current Infrastructure of the STDCThe STDC is a three-story residential building and a functional basement with training/seminar room facilities, a separate computer room, residential rooms, kitchen and dining area etc. and a waiting room along with rooms for STDC staff including medical officers and a library. The ground floor has rooms for administrative persons, the kitchen and dining area, the first floor has training rooms (three Nos.), individual residential rooms and an open terrace with seating arrangement while the third floor houses the dormitories for male and female residents. All floors have washroom areas (separate toilets for males and females) and a drinking water cooler. The basement is largely used for storage purposes. The building has a lot of open area and a boundary wall. There is a small garden and kitchen garden within the premises. A detailed description of the infrastructure is provided below.
Rooms used for Training Purposes
The STDC has three kinds of rooms that are used for training purposes:
1.Seminar hall:
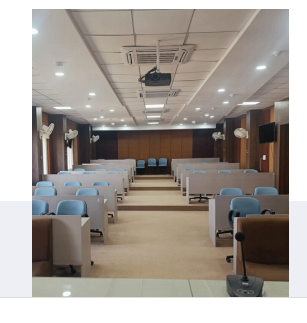
The biggest room is the seminar hall which is a 50 seated hall in a gallery style that also has a dais with a podium for all large sized trainings and other formal programs at the STDC. The gallery also has an interactive smartboard and three LED screens that are located strategically within the hall so that all participants have a proper view of the projection made on the smart board. The hall is also equipped with a good sound system including mics and an amplifier and a projector. The walls are panelled for sound proofing as well as for amplification and the floor is carpeted to reduce additional noise. There are four ACs in the seminar hall and an attached bathroom for males and females as well as a water cooler stationed right outside the hall.
2.Computer room:

The second hall is the computer lab which is smaller in size than the seminar room. This hall has designated desks and benches with computers (15 Nos.), screen and a smartboard with a stable internet system in place. The room has two ACs fitted. This room is primarily used for training cadres which require participants to use computers themselves during the training process (eg: medical officers and nurses).
3.Conference hall:

The smallest of the three training halls is the conference room. This room is designed to hold closed door meetings among small groups. It consists of a meeting table with a 20-seater seating arrangement around the table with an additional 20-seater arrangement. Other facilities in this room consists of a screen, LED and a hanging projector.
4.Residential Facilities:

The STDC, Bhopal, has hostel accommodation within the STDC building for those who attend training programs at the STDC. There are a total of 12 rooms at the STDC (8 rooms are on a double occupancy basis; 4 rooms are on a triple occupancy basis). A total of 28 persons can be accommodated in these rooms. In addition, there are two dormitory rooms (one for males and one for females). Each of these dorms have an arrangement of 10 beds with attached bathrooms, running hot water. All rooms for residential purposes have ACs, sufficient number of bathrooms with running hot water and provision for a common washing machine as well as laundry services on a self-payment basis. The rooms and dormitories are provided with appropriate number of study tables, chairs, wardrobe, a small pantry and a dressing table. All the rooms and the dormitories are well ventilated.
5.Dining Facilities:

The STDC has a large dining area and a fully functional kitchen that can cater between 50-60 persons at a point in time. The dining area has a seating arrangement for 40 persons at a time. There is a large sized fridge and a microwave in the kitchen/dining area for the purpose.
6.Rooms available for Administrative purposes by STDC staff:

There are dedicated rooms for the STDC director, medical officers and other staff of the STDCs. In addition, there are two rooms for administrative purposes of which one room has the Echo hub set up for meetings. There is a small library section in the second administrative room.
7.Other facilities/provisions available at the STDC:

The STDC has a solar panel with a capacity to generate 5 Kilowatts of energy equivalent electricity, regular water supply, steady internet (fibre plan of 40 GB) and routers in each floor for improved connectivity, and provision for a landline telephone connection. The expenditure incurred for electricity, internet and water is funded through the State Health society.
8.Human Resource available at STDC:

Currently, the STDC (including the IRL) has a total of 26 staff in place against a sanctioned human resource of 47 persons. The NTEP program provides 9 staff while 13 support staff (contractual) is provided by the NHM. The rest of the staff is positioned through the State health society.
9.Provision for Maintenance and Upkeep of the STDC:

While the STDC had received grants to set up the infrastructure across years, the regular maintenance and upkeep of the infrastructure is supported through income generated from hosting trainings for health cadres other than the NTEP staff. These include trainings conducted for ASHA, ANMs, nurses and Medical officers from block level facilities. The training halls and residential facilities are rented out to generate income that is used for regular maintenance of the building.
Key Learnings
Key Learnings
The primary learning from the establishment of the STDC, Bhopal, has been the high level of commitment shown by the senior authorities in prioritizing the establishment of the STDC, Bhopal. It is evident from the interviews conducted with multiple stakeholders at the state and review of relevant government documents that the importance of establishing a proper infrastructure for STDC was a ‘felt need’ by the senior officials to establish the NTEP program and improve on the quality of the service provisioning. This was in the context that the STDC staff were operating out of the two rooms from the TB hospital prior to the establishment of the STDC infrastructure. This impacted their ability to conduct regular trainings for the NTEP staff even as the program was expanding in the state and knowledge of the TB program was growing simultaneously.
Once the vision to establish the STDC was rolled out, it is important to note that the state ensured close supervision through the medical officers who were tasked to follow up on the construction and completion of the infrastructure. The entire process from conceptualizing to the construction of the building by different departments under the overall supervision of the highest official in the state for health worked to support each other to establish this institution building.


“The NTEP program in Madhya Pradesh has evolved immensely over the years and the establishment of an independent STDC building has added value to the optimal functioning of the program. As the program has evolved through the years, the NTEP cadre and their functions have also changed requiring them to be trained on the latest and updated knowledge. A designated residential training centre equipped with the latest technology and infrastructure has been key in ensuring a trained NTEP staff in the state contributing towards enhance program activities and outcomes. I hope other states in the country are encouraged from the story of the establishment of STDC, Bhopal and initiate their own STDCs”.
Dr. Varsha Rai,
State TB Officer, Madhya Pradesh
NTEP
STDC Agra,UP- From Planning to Practice: State TB Supervisor Training in Uttar Pradesh
STDC Agra,UP- From Planning to Practice: State TB Supervisor Training in Uttar PradeshSTDC Agra ensures uniform training covering over a thousand STS through meticulous planning
BACKGROUND:
The National Strategic Plan (NSP) 2017–2025 of the NTEP emphasizes that an "adequately staffed, trained, and motivated health workforce is essential to achieving the ambitious goal of ending TB.” In line with this vision, the NTEP envisaged the STDCs playing a significant role in building capacities of the NTEP cadres, General Health System and Private health care facilities/providers, along with SM&E of the programme and Operational Research. A key focus of the training strategy defined in the NSP for the programme is to not only to close gaps by addressing the need for a fully trained workforce but also to create a sustainable model that keeps staff updated on evolving policies and guidelines. This ensures the continuous flow of accurate information across all levels of NTEP personnel.
The Guidelines and Norms for STDCs in NTEP 2023, further underscore this responsibility, stating that ‘STDCs are expected to build the capacity of HRs in the programme, i.e., NTEP key personnel, general health system, medical college faculty and private health sector in relation to programme operations so that they are able to effectively deliver TB services and execute the roles expected from them.’ The guidelines recommend regular in-depth training at the time of staff induction, supplemented by updates as needed. Moreover, STDCs are tasked with preparing comprehensive training calendars annually and supporting district-level planning to align with the state’s Program Implementation Plan (PIP).
Recognizing this critical role, STDC Agra, meticulously planned and executed the uniform training of all 1017 Senior Treatment Supervisors (STS) in a two-year period, in line with the Guidelines and Norms for STDCs 2023. This document outlines the meticulous approach taken by STDC Agra to achieve this, highlighting the key steps in planning and delivering effective training that aligns with national priorities.
The Process
The ProcessThe task of training 1017 Senior Treatment Supervisors (STS) across the state demanded a well-coordinated and strategic approach from STDC Agra. To meet this challenge, the team developed a robust and comprehensive plan that laid the groundwork for successful implementation. This roadmap focused on gathering detailed trainee data, scheduling training batches, and ensuring timely communication and resource allocation. The planning phase set the stage for a seamless execution of the training program, ensuring every STS received the necessary knowledge, skills and support to contribute to the programme.
1. Planning
For ensuring uniform training of 1017 STS in the state, STDC Agra resorted to robust planning.
The first step was to create a comprehensive roadmap inclusive of following steps:
•Collection of Trainee information: The team meticulously crafted a detailed list of all STS personnel across the state, categorized by district. This was done based on the training planning tool prepared by Central TB Division (https://ntep.in/node/3614/BookPage/25-planning-tool) in collaboration with USAID supported The Union led iDEFEAT TB Project. This served as the denominator.
•Create Batches as per the resources available: Based on the infrastructure, dates and resource persons available, STDC Agra created batches for imparting the trainings.
•Assign Trainees to the various Batches: They assigned trainees to the various batches. Each training batch was scheduled perfectly to ensure the participation of every STS. Batches were created keeping in mind that the work on the ground is not to be affected. At the same time, STDC team ensured that no one was left behind.
•Communication/ Invitation to Trainees: Requisite and timely communication was sent out to the trainees allowing sufficient time to be prepared for taking the batches.
•Identification of the resources required for training: Medical Officers of the STDCs and WHO-consultants served as the resource persons for these training sessions. Resource persons were meticulously mapped against each batches to ensure their availability. Funds for the trainings were budgeted in Program Implementation Plan (PIP).1
•Localized Learning: Course for STS on NTEP approved by Central TB Division was a 40-hour curriculum including 11 modules and 43 chapters (https://ntep.in/node/3408). To enhance the understanding, STDC translated training materials into Hindi, making the content accessible for participants from diverse educational backgrounds.
2. Operationalizing:
STDC organized 32 training sessions for covering 1017 STS over two years, from August 2022 to April 2024. Out of these, 8 batches were undertaken using the modernized training system. The Modernized Training system entailed use of blended mode of classroom training such that the training was imparted using virtual technological mechanisms.
•Role of Training Co-ordinator: A dedicated training coordinator was appointed to oversee the entire process from start to finish. Their responsibilities included meticulously planning the training schedules in close collaboration with the State TB Cell and STDC, selecting and assigning facilitators, and ensuring the necessary resources—such as training venues—were in place. Additionally, the coordinator was tasked with organizing training batches, scheduling courses within the Learning Management Information System, monitoring the progress of the trainings, and keeping all key stakeholders regularly updated. This comprehensive role ensured smooth and efficient execution of the training program.
•Practical learning: The training was highly practical and immersive, featuring six-day induction sessions complemented by two-day refresher courses. Emphasis was placed on real-world applications, allowing participants to actively engage with the material. This hands-on approach not only deepened their understanding but also boosted their confidence in effectively applying newly acquired skills within their respective districts.
•Continuous Monitoring: The STDC assessed the effectiveness of the training by conducting pre- and post-tests through the Learning Management System (LMS), allowing for data-driven insights. Feedback was actively incorporated, enabling session adjustments to ensure continuous improvement and enhanced learning outcomes.
•Inclusivity at Its Core: The STDC created an accessible and supportive training environment by providing accommodations, meals, and logistical assistance for all participants, including individuals with disabilities. These efforts ensured an inclusive atmosphere, allowing everyone to fully engage in the learning experience
•Collaboration: The trainings were undertaken in collaboration with WHO NTEP Technical Support Network and The Union led iDEFEAT TB Project.
•Team Work: Under the chairpersonship of Director, STDC staff coordinated and implemented the training activities with a clear roles and responsibilities.
1. In the context of public health programs in India, especially under schemes like the National Health Mission (NHM), a PIP refers to a detailed annual plan that outlines the activities, interventions, budgetary allocations, and goals for implementing specific health programs at the state or district level.
Conclusion
ConclusionThe role of STDCs in building the capacity of NTEP personnel is pivotal to achieving the goals set forth by the National Strategic Plan 2017–2025. Through effective training and continuous updates, STDCs ensure that all cadres of NTEP staff are well-equipped to deliver high-quality TB care. STDC Agra’s meticulous planning and execution of training for 1017 Senior Treatment Supervisors over a two-year period serves as a prime example of how a structured, well-coordinated approach can successfully align with national priorities. STDC Agra has demonstrated the critical impact of robust training in enhancing TB service delivery and contributing to the broader goal of ending TB in India.
"Our success in delivering effective STS training in Uttar Pradesh was rooted in a systematic approach. First, we collected a detailed line list of all STS across the state. Then, we distributed responsibilities and ensured accountability for every task. Each team member had a specific role, whether it was planning the batches, addressing participant queries, or maintaining the training environment. We mobilized resources, created WhatsApp groups, and ensured seamless coordination—right from sending welcome emails to arranging guest lectures and hospitality. Every trainer was handpicked, and we had a dedicated person overseeing the entire training process. Finally, gathering feedback became essential for quality assurance and continuous improvement. This structure allowed us to deliver consistently high-quality training for all 75 districts for STS cadre”.
Dr.Sanjeev Lawania, Director, STDC Agra
STDC Delhi- Operational Research under NTEP: Learnings from New Delhi Tuberculosis Centre
STDC Delhi- Operational Research under NTEP: Learnings from New Delhi Tuberculosis CentreINTRODUCTION
India accounted for more than 25% of the global TB burden. To End TB, various interventions are planned by the Centre and State under the National Tuberculosis Elimination Program (NTEP).1 Operational Research is one of the requisites to generate continuous evidence to ensure state strategies are aligned well with the National Program. This evidence informs change in interventions or policy and optimize implementation of program activities to improve overall health outcomes.2
The National Strategic Plan for TB Elimination in India encourages and promotes Operational Research (OR) activity. Central Tuberculosis Division (CTD) has published areas and priorities for operational research at state, zonal and national level. The ‘Revised Norms and Guidelines for STDC’3 recommend STDCs to independently plan and execute need-based operational/implementation research and inform effectiveness of interventions at State.
However, most of the STDCs in the country are unable to conduct research activities due to underlying deficiencies in the systems or capacities. STDC Delhi has been conducting research studies regularly. Most of the projects have been conducted in collaboration with Indian Council of Medical Research (ICMR), National Institutes for TB, Medical colleges at New Delhi, Delhi TB-Association and development agencies like FIND (the global alliance for diagnostics), The UNION (International Union Against TB and Lung Disease), MRC-London (Medical Research Council), Centre for Equity etc. Around one-third of the total research projects undertaken by STDC Delhi in past 7 years are Operational research projects.
Since 2016-17, 102 research projects have been published as formal research papers, 56 of them have been published in the past 3 financial years. Some of the findings from these research studies have been incorporated into practice under NTEP. Findings from studies like National Sample survey for TB in 1950, eight longitudinal disease prevalence surveys conducted in domiciliary area of STDC Delhi for over 30 years, Active Case Finding (ACF) campaign in homeless pavement dwellers along Yamuna Pushta with mobile X-ray van supported by Medanta Medicity in Gurugram4 and prevalence of initial and acquired drug resistance and outcomes of Short-course chemotherapy (SCC) are some of them.
STDC Director and the staff has participated in 889 scientific events in last decade (since 2014-15) which has resulted in collaborations, cross-learning, funding and more research opportunities. The staff has gone an extra mile in presenting their research projects and findings at National (19) and International (13) scientific platforms. This document captures the experiences of STDC Delhi in conducting an operational research and key learnings. The enabling factors are listed in detail as an information for other STDCs to enhance replication and uptake.
STDC Delhi
Established in 1940 by Government of India and TB Association of India4 (TAI) jointly, officially known as New Delhi TB Centre (NDTBC) functioned as a model clinic for initiating organized domiciliary treatment for TB. In 1951, the center upgraded to first TB Training and demonstration center (TDTC) to provide training to health care workers and diagnostic referral center for five northern states until formal declaration as an STDC in 2005. Since then, STDC Delhi has been actively promoting operational research with the prime objective of evolving patient friendly and cost-effective treatment to people with TB. The details of the research activities and projects may be assessed from the annual reports published by STDC Delhi.4
1.https://tbcindia.mohfw.gov.in/wp-content/uploads/2023/06/5646719104TB_A…
2.theunion.org/sites/default/files/2024-06/Union OR to Improve Health Services 2nd 2024.pdf
3.https://tbcindia.mohfw.gov.in/wp-content/uploads/2024/08/Norms-and-Guid…
4.https://www.ndtbc.com/annual-report
Enabling Factors For Conducting Operational Research at STDC Delhi
Enabling Factors For Conducting Operational Research at STDC Delhi1.Human Resource: STDC Delhi developed its full-fledged sections in epidemiological, public health, statistical and administrative wing. The STDC director provides leadership and guidance to opportunities for conducting research. The Epidemiologist at STDC serves as the nodal officer for implementation of research. He is supported by a microbiologist and a biostatistician for monitoring collection and analysis of research data.
2.Capacity Building on OR: The key staff along with STDC Director completed their formal training in research methodology in 1990 and ‘How to do Operational Research?’ in 2005 at National Tuberculosis Institute, Bangalore.
3.Financial Resources: Along with funds earmarked for operational research in State NTEP funds, STDC Delhi shares experience of trying odds with every opportunity to fund its research. In last 10 years, more than 50% of the total researches were funded by State Operational Research Committee. In addition, some research projects are funded by ICMR or external agencies like MRC London, Corporates like Sandoz under corporate social responsibility (CSR). Funds earmarked for research studies are restricted to use under the same functional component.
4.Infrastructural capacity: Accredited with National Accreditation Board for Testing and Calibration Laboratories (NABL), the Intermediate reference laboratory (IRL) at STDC Delhi is equipped with Biosafety Level-3, Whole Genome Sequencing (WGS), second-line Line Probe Assay (LPA) and Liquid culture DST (drug-susceptibility testing) facilities. These make STDC Delhi a preferred site for research projects meant for multi-centric clinical trials, kit validation or validation of new diagnostic modalities4 in collaboration with RBIPMT (The Rajan Babu Institute of Pulmonary Medicine and TB), NITRD (the National Institute of TB and Respiratory diseases) or NIRT (National Institute for research in Tuberculosis, Chennai).
5.Orientation to potential researchers: STDC Delhi regularly conducts orientation workshops for potential researchers (DTO), faculty from various medical and nursing colleges, development agencies and corporate entities to sensitize on potential areas for operational research. Guidance on research tools to support good quality data collection is circulated.
6.Institutional mechanisms: STDC Delhi has established an institution level 7-member Scientific Advisory Committee, that reviews and finalizes the research proposals to be submitted to Operational research committee on behalf of STDC Delhi.
STDC Delhi has its own Institution Level Ethics Committee4 with members represented from TB Association of India, Delhi TB Association, State level Legal advisor, Community member, STDC itself and chaired by a Medical College faculty. The committee reviews the submitted protocols and provides ethical clearance based on the type of research involved.
7.Collaboration with State OR mechanism: STDC Delhi remains the focal point for organizing state task force meetings. The State Operational Research committee meets at STDC Delhi regularly to review and finalize the submitted proposals. Hence, any upcoming/ ongoing research is informed to STDC Delhi and priorities for conducting the same is facilitated. The State Task force also advocates for one thesis per medical college in a year to be undertaken by postgraduates.
8.Collaboration with TB Association of India (TAI): The staff of STDC Delhi provides managerial support to TB Association of India. They support the publication of the quarterly journal of TAI as members of editorial board4. Also, the faculty actively participates in annual conferences organized by TAI and supports in finalizing the scientific program and participating in the sessions. This provides an opportunity for STDC Delhi to create more awareness in their staff regarding current priorities of the national program, learnings from other states and dissemination of their research findings.
9.Maintaining a database of research studies: STDC Delhi documents the database (offline & online) of TB related (past and ongoing) research activity conducted in state. It is maintained as a part of the program annual report documented by STDC. It helps in wide dissemination of undergoing projects and provides an opportunity for collaboration, cross-learning or enhancement of research. Details of the research projects taken up in 2022-23 are listed in the annexure.
10.Dissemination of findings: STDC Delhi encourages use of various media to disseminate their research findings to the community at large. Around two-thirds of the total publication (71) is disseminated each through research publication or review article in past 6 years. This helps to keep the team motivated and continue to uptake further research projects.
Key Learnings
Key LearningsInvolvement of District Tuberculosis Officers: STDC Delhi encourages participation of District Tuberculosis officers (DTO) in conceptualization of research topics, implementation of research, training the project staff and monitoring the data collection. Inclusion of DTOs in the research team lays off any administrative issues related to data collection and absorption of research findings into practice.
Technical expertise from Medical College: STDC Delhi actively participates in approaching Medical College faculty for their technical expertise. Many research projects are planned in the form of thesis/ research work/dissertation as a part of the students’ medical programme curriculum. Having principal investigators or co-lead from the medical college adds value to the research topic and benefits the programme.
Supervision and Monitoring: Frequent supportive supervisory visits are conducted by STDC staff in the project area. The challenges in implementation are discussed and strategies are realigned, if necessary. The State OR committee regularly conducts mid-term review of the ongoing research studies.
Sustainable and resilient systems: STDC Delhi have worked around creating and sustaining institutional mechanisms that are not individual dependent. The processes for conducting an operational research at STDC Delhi has evolved and defined with time. It is elaborated in diagram below. Any operational research in the State is well informed to STDC and every activity is well coordinated with support from State TB Cell. The steps include collaboration with multiple stakeholders and their technical experts. Mechanisms to receive funds for research projects are well identified for smooth disbursement.
Process flow diagram for conducting Operational Research at STDC DELHI
Process flow diagram for conducting Operational Research at STDC DELHI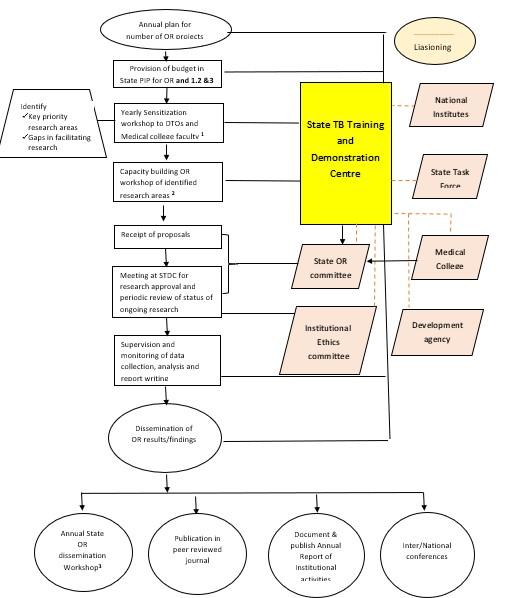
Few challenges on timely release of funds due to delay in in receipt of utilization certificate from other institutions have been reported. The STDCs need to anticipate such challenges and be prepared accordingly for smooth completion of research.
List of research activities supported by STDC Delhi in 2022-23
List of research activities supported by STDC Delhi in 2022-23|
S.no |
Title |
Study area |
Type of research |
Source of funding |
|
1 |
Mapping of Anti-Mycobacterial Drug Resistant Hotspots under NTEP in Delhi State |
STDC Delhi & TAI |
Operational Research |
Delhi State OR Committee |
|
2 |
TB prevalence & interventions for reducing TB and LTBI in high-risk key population of rickshaw driver & construction workers |
Selected districts of Delhi |
Operational Research |
ICMR |
|
3 |
Prevalence, risk factors and laboratory diagnosis of non-tuberculous mycobacterial (NTM) disease: A multicentric study |
IRL, STDC Delhi and 5 other sites in country |
Multi-centric trial |
ICMR |
|
4 |
Short intensified treatment for children with tuberculous meningitis (SURE) |
IRL, STDC Delhi and Kalawati Saran Children hospital, New Delhi |
Clinical Trial |
MRC, London, UK and National Institute of Health Research |
|
5 |
Evaluate the effectiveness, safety and tolerability of various Linezolid in combination with Bedaquiline and Pretomanid in Adults with Pre-Extensively Drug-Resistant or Treatment Intolerant/Non-responsive Multidrug-Resistant (MDRTI/NR ) Pulmonary TB in India. |
IRL, STDC Delhi and RBIPMT, New Delhi |
Clinical Trial |
ICMR |
|
6 |
Assessment of effectiveness of the 4-month Moxifloxacin containing daily regimen in the treatment of microbiologically confirmed new pulmonary TB patients |
IRL, STDC Delhi and TB Chest clinic at Lok Nayak Hospital |
Clinical Trial |
ICMR |