Content Status
Type
Linked Node
Management of DR-TB ADR: Gastrointestinal Symptoms [Nausea and Vomiting]
Learning Objectives-
Mild to moderate nausea and vomiting lasts 1-2 days without any associated symptoms and is managed conservatively at home, with telephonic consultation to the Drug-resistant TB (DR-TB) centre.
Repeated vomiting exceeding a day or two with signs of severe dehydration and discomfort is a serious presentation of this ADR which should be referred to the nearest DR-TB centre.
Suspected agent(s): Ethionamide (Eto), P-aminosalicylic Acid (PAS), Pyrazinamide (Z), Ethambutol (E), Bedaquiline (Bdq)
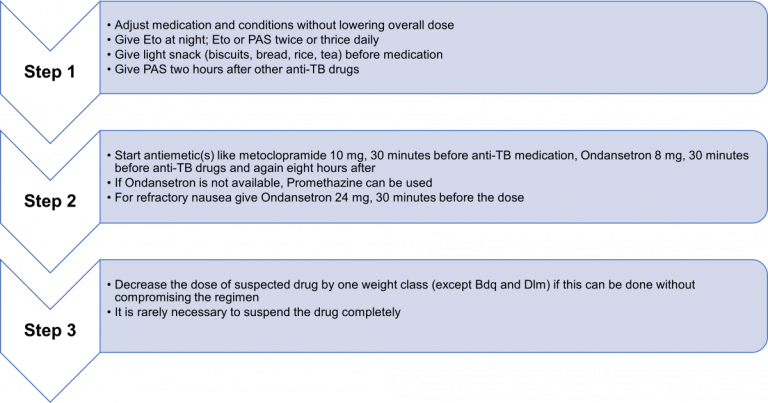
Suggested Management Strategies
- If there is nausea or vomiting: Take drugs embedded in a banana.
- If vomiting persists: Administer drugs 1 hour after 1 tablet of Domperidone and/or Omeprazole or Famotidine/ Ranitidine. No other antacids should be given since they interfere with the absorption of Fluoroquinolone (FQ).
- For severe vomiting:
- Monitor the patient’s hydration status
- Assess patient for danger signs including dehydration and electrolyte disturbance
- If required, initiate rehydration treatment and correct electrolyte disturbances
- Temporarily withhold drugs, and conduct tests to rule out other causes of vomiting like hepatitis
If there is blood in the vomit: Check haemoglobin and treat for possible bleeding ulcers
If the offending drug is Ethionamide (Eto): Administer it with milk or at bedtime to avoid nausea.
With Bedaquiline (Bdq), Metoclopramide is preferred over Ondansetron; and Ranitidine is preferred over Omeprazole.
Points to Note
- Nausea and vomiting are universal in the early weeks of treatment and usually abate with time on treatment and adjunctive therapy.
- Some nausea and even vomiting may need to be tolerated at least in the initial period.
- Creatinine and electrolytes should be checked in case of severe vomiting. Give intravenous fluids and replace electrolytes as needed.
- Another strategy is to stop the responsible medicine for 2-3 days and then add it back, gradually increasing the dose (advise the patient that the medicine will be increased back to a therapeutic dose in a way that is better tolerated).
- Ondansetron prolongs QT interval; avoid the use of ondansetron with Bdq or Dlm.
- For patients particularly anxious about nausea, (and with “anticipatory nausea and vomiting”) a small dose of an anti-anxiety medicine (5 mg of diazepam) can help when given 30 minutes prior to intake of anti-TB drugs.
Resources
Content Creator
Reviewer
- Log in to post comments